Berberine inhibits the proliferation of human uterine fibroid cells
Berberine inhibits the proliferation of human uterine fibroid cells
Treatment of fibroid cells with berberine inhibited cell proliferation by approximately 60%.
COX-2 is a critical enzyme that converts arachidonic acid into prostaglandin E2 (PGE2) and is commonly overexpressed in many solid tumors, including colorectal, breast, prostate, and ovarian neoplasms.
Increased expression of COX-2 and the associated PGE2 production have been demonstrated to significantly enhance carcinogenesis. Ke et al. reported that COX-2 expression was significantly up-regulated in uterine fibroids and that the inhibition of COX-2 activity significantly reduced the proliferation of the uterine fibroids smooth muscle cells, which suggests that COX-2 is involved in the pathogenesis of uterine fibroids.
In turn, berberine has been reported to induce cancer cell apoptosis and suppress cancer cell migration in many neoplastic cell lines, including melanoma, non–small cell lung cancer (40), and oral cancer, an effect mediated through the reduced expression of COX-2.
Consistent with these observations, our data indicate that BBR significantly reduced COX-2 expression in uterine cells, which suggests that COX-2 may also play a role in mediating BBR-induced apoptosis in human uterine cells.
Berberine inhibits the proliferation of human uterine fibroid cells
The controlling factor in fibroids is excess oestrogen producing oxidative stress (inflammation) causing DNA damage which goes on to cause symptoms. The shrinking of fibroids depends on reducing oestrogen levels, repairing DNA damage with vitamin D and managing inflammation with antioxidants.
Fibroids are the most common growths in the uterus. Their growth is stimulated by oestrogen and progesterone, causing uterine collagen to cross-link and harden, creating a stiff mass of collagen fibres. Fibroids tend to develop in early perimenopause, when oestrogen levels increase and regress in menopause as oestrogen declines. Fibroids tend to have more oestrogen receptors, so this may be one reason oestrogen disproportionately affects the growth of these solid tumours. More than 80% of Black women and nearly 70% of white women have fibroids by age 50. Sometimes these growths are harmless and can even go undetected, but in many cases they cause symptoms ranging from pain and bleeding to infertility.
1. Early warning signs
The symptoms of fibroids are relatively common and can be associated with other factors or diseases, such as ovulatory dysfunction, endometriosis or endometrial polyps. Many women do not connect their symptoms to fibroids, so can go undiagnosed for some time, and some fibroids can be asymptomatic, thereby avoiding detection. Many women have uterine fibroids and don’t even know it. Small fibroids don’t often cause symptoms and don’t regularly affect your life. However, larger fibroids may lead to several warning signs, including:
Heavy bleeding: you can experience heavy menstrual bleeding, large clots, and bleeding between cycles when you have one or more uterine fibroids. This is the most common symptom. Excessive bleeding can lead to the development of anaemia (low red blood cells) causing ongoing tiredness and weakness.
Pelvic pressure or pain, lower back pain: pelvic pain and low back pain are common early symptoms of uterine fibroids. The pain may be sharp or feel similar to your menstrual cramps but worse.
Full feeling in the abdomen: as uterine fibroids grow, they occupy more space in your uterus and pelvic area. You may feel like your belly is full, as if you’ve eaten a large meal.
Increased urination: you might feel like you have to urinate more often when you have uterine fibroids. This happens when the fibroid is big enough to put pressure on your bladder. Although rare, fibroids can also cause obstruction of the ureter, which might require treatment if this progresses to severe hydronephrosis.
Pain during sex: the fullness in your abdomen that fibroids cause can also lead to discomfort during sex. Not everyone feels this, but if you have pain with intercourse, getting evaluated for uterine fibroids is a good idea.
Gastrointestinal symptoms: constipation or the recurrent need to void bowels can also be caused by fibroids.
Rarely, a fibroid can cause sudden, serious pain when it outgrows its blood supply and starts to die. Get medical care right away if you have severe bleeding from the vagina or sharp pelvic pain that comes on fast.
There are long-term complications that can affect the integrity of the endometrium, the uterine lining. This means it can be difficult getting pregnant. During pregnancy, women with fibroids have an increased risk of complications compared with women without fibroids, including
preterm delivery (16.7% versus 6.3%) and
premature rupture of membranes (14.3% versus 2.1%)
risk of placental abruption (7.5% versus 0.9%)
fetal malformation (6.2% versus 3.3%)
caesarean section (70–76% versus 32.8%)
postpartum haemorrhage (33% versus 6%) and
foetal malpresentation (19% versus 4.4%) are increased in women with fibroids
Fibroids can also be associated with miscarriage.
The symptoms of fibroids are relatively common and can be associated with other factors or diseases, such as ovulatory dysfunction, endometriosis or endometrial polyps. Many women do not connect their symptoms to fibroids, so can go undiagnosed for some time, and some fibroids can be asymptomatic. Lack of symptoms does not necessarily mean lack of inflammation, so women experiencing infertility should be evaluated to the presence of fibroids.
2. Presentation and Diagnosis
Diagnosing fibroids is usually done by transvaginal ultrasound, although this is limiting if the uterus extends beyond the pelvis, a common problem with this disease. Abdominal ultra-sonography might be required to diagnose fibroids that extend beyond the effective range of the trans-vaginal probe, but then MRI is generally preferred.
Women often have more than one fibroid. They can be different in size and in their location. The location of fibroids directly affects the symptoms they induce, as well as the time to the manifestation of such symptoms. For example, submucosal fibroids that bulge into the uterine cavity seem to have more of an effect on abnormal menstrual bleeding and pregnancy problems. This is independent of fibroid size as small fibroids that protrude into the uterine cavity can also induce menstrual irregularities. Conversely, subserosal fibroids that form on the outside of the uterus are slow growing and considerable time is needed before they are of a sufficient bulk to cause symptoms, such as back, leg or pelvic pressure and abdominal and pelvic pain.
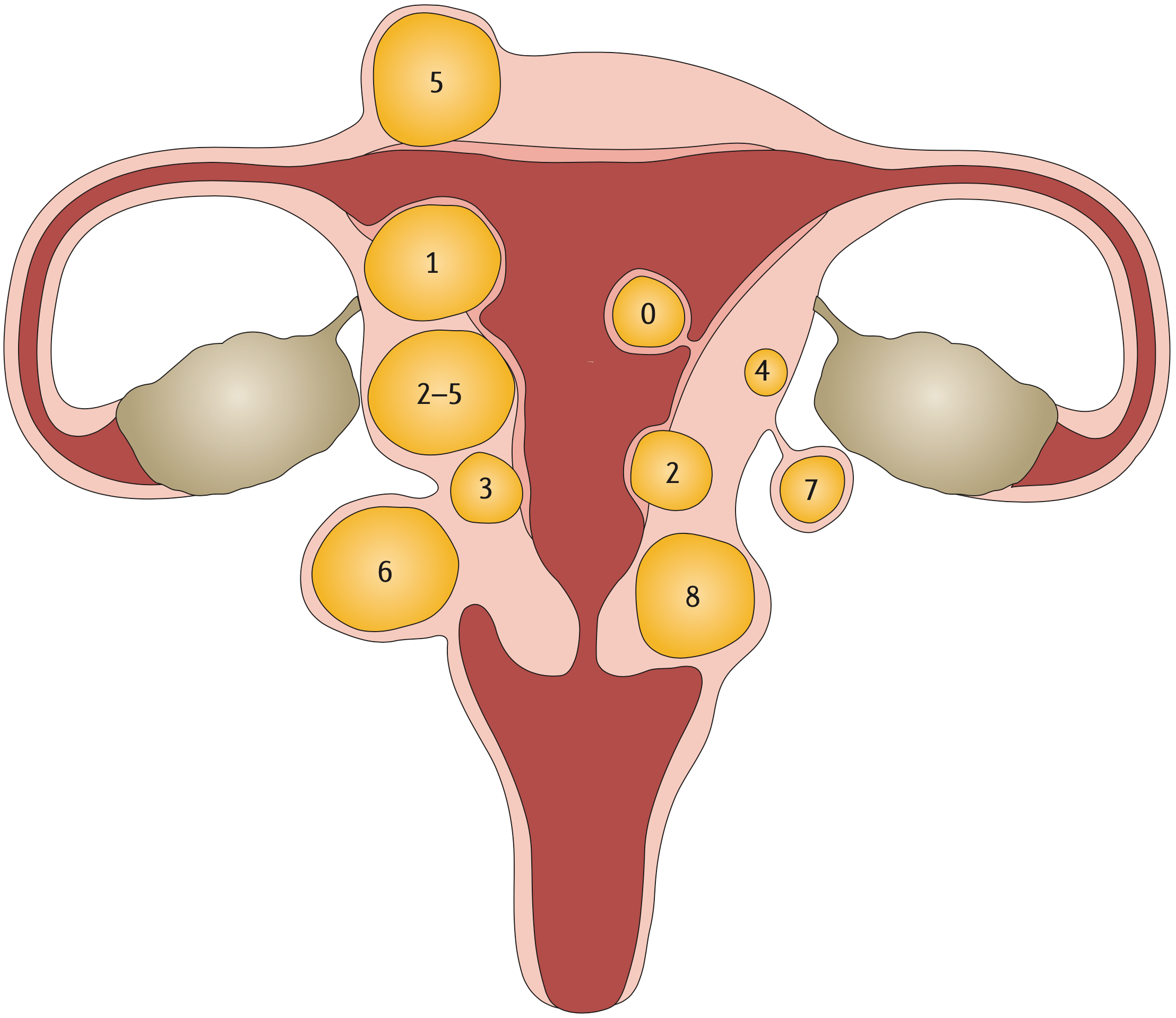
The International Federation of Gynecology and Obstetrics (FIGO) has established a classification system which uses an 8-point numerical system to describe the location of fibroids relative to the endometrium (submucosal surface) and the serosal surface, with low numbers indicating a central location.
Type 0: pedunculated fibroid, which is localized in the submucosa and extends inside the uterine cavity
Type 1: submucosal fibroid, with <50% in an intramural location
Type 2: submucosal fibroid, with ≥50% in an intramural location
Type 3: contacts the endometrium, with 100% in an intramural location
Type 4: intramural fibroid
Type 5: subserosal fibroid, with ≥50% in an intramural location •
Type 6: subserosal fibroid, with <50% in an intramural location •
Type 7: subserosal pedunculated fibroid
Type 8: other (for example, cervical or parasitic)
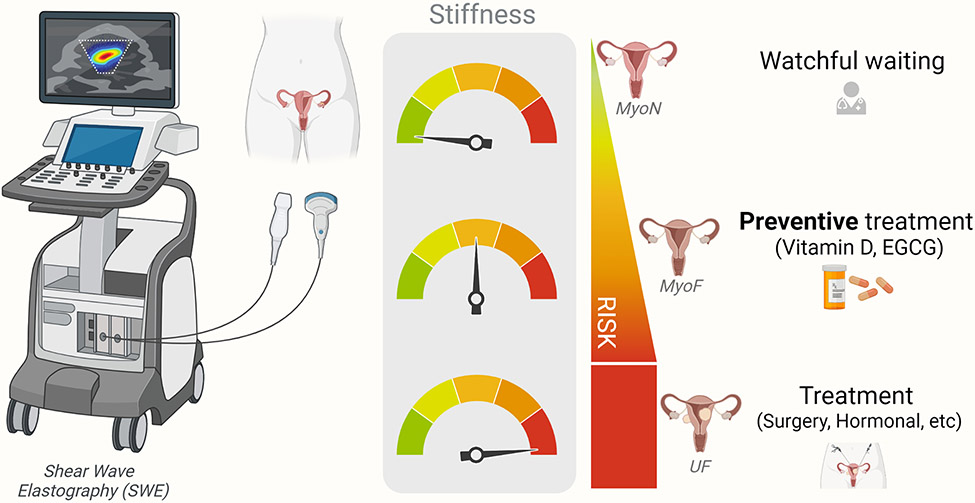
Proposed application of SWE as a screening tool for identification of women at risk of fibroid development and corresponding preventive measures to be taken. MyoN: normal non-fibroid myometrium; MyoF: at risk-myometrium, EGCG: Epigallocatechin Gallate.
The principle of SWE is to use sound waves to produce images. The sound waves can give an indication of how stiff the uterine tissue is: soft, firm, solid or hard. The stiffness indicates the progression of fibroid growth, as well as the use of appropriate therapies.
3. Biomarkers
In urine
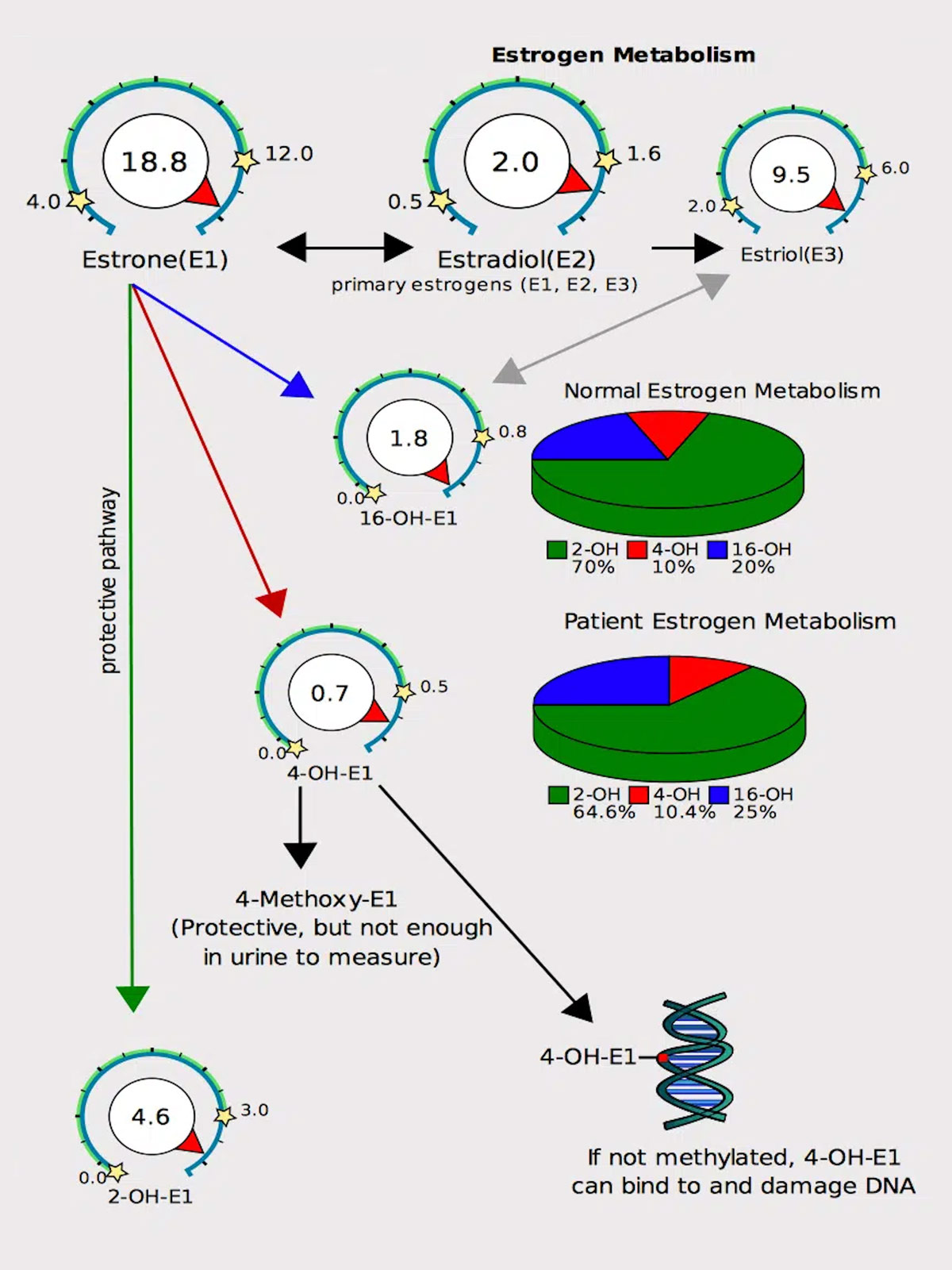
As oestrogen can fuel the growth of fibroids, it can be helpful to identify whether oestrogen is elevated, and how it’s metabolised. DUTCH urine testing is unique because it helps identify symptoms of hormonal imbalances by providing a complete picture of hormone levels which cannot be seen in testing serum (blood) alone. The DUTCH test can measure the levels of the 3 types of oestrogen, oestrone (E1), oestradiol (E2) and oestriol (E3) and how they are metabolised.
Estradiol (E2) is the most biologically active estrogen in the body. However, estrone (E1) and the phase 1 estrogen metabolites (2-OH, 4-OH, 16-OH) can also bind to estrogen receptors. Thus, it is possible that elevations in any of these markers may contribute to fibroid growth.
The phase 1 metabolite, 16-OHE1, tends to bind more tightly to oestrogen receptors than the 2-OH and 4-OH metabolites (but not nearly as tightly as E2), and is known to cause tissue groeth. If too much oestrogen is metabolised into the 16-OHE1 form, it may contribute to increased fibroid growth.
Having this information is extremely valuable, because it means that as a practitioner I can first reduce the amount of oestrogen and alter the metabolism of oestrogen in a more favourable way.
In blood
The CA-125 blood test measures the amount of CA125 protein that both women and men have in their blood. CA-125 is elevated in cases of fibroids, endometriosis and adenomyosis, as well as ovarian cancer. This means that it can’t be used to identify any one of these conditions, but it can be used to monitor progression.
4. Development and Progression of Fibroids
Fibroids are associated with high oestrogen levels, or oestrogen dominance. Obesity and the perimenopausal state are often associated with higher oestrogen levels. Studies have shown that oestrogen levels are actually higher in perimenopausal women, and fat is hormonal organ capable of producing oestrone, a strong oestrogen. The inflammatory mediators interleukin-2 (IL-2), IL-6, tumor necrosis factor-alpha (TNF-alpha), and leuko- triene B4 (LTB4) are also produced in the adipocyte and contribute to fibroid formation.
MED12 gene mutations created by high oxidative stress in the uterus drive fibroid formation
Nearly 70 percent of uterine fibroids are linked to a mutation in the MED12 gene but recreating this problem in the lab has proven to be difficult because when cultured, the mutant cells in the fibroids do not survive. This year scientists used CRISPR-based genome editing technology (for which 2 women scientists won a Nobel prize in 2020) to precisely engineer cells that have the same mutation in the MED12 gene. After successfully culturing the mutated fibroid cells in 3D spheres, it was found that the cells produced heightened levels of collagen, a key feature of uterine fibroids, as well as other chromosomal abnormalities commonly seen in uterine fibroids.
A clear connection has been made between MED12 mutations and high levels of oxidative stress in the uterus. The direct connection between oxidative stress and MED12 is not yet clear however almost all the risk factors below can drive oxidative stress.
What is oxidative stress?
Biochemical reactions in the body leave toxic residues – (commonly known as reactive oxygen species or free radicals) – that can damage cellular components such as DNA, proteins, and lipids. Antioxidants can neutralise free radicals and repair damage. In a healthy state, the body maintains a balance between the generation of free radicals and the antioxidant defences that neutralise them.
When the generation of reactive oxygen species overwhelms the body’s antioxidant defences, oxidative stress occurs. This imbalance can result in cellular and tissue damage,
Several factors, including environmental pollutants, smoking, poor diet, and physical stress, can lead to an overproduction of these reactive oxygen species.
5. Risk Factors
Anything that increases oestrogen:
Age Increasing age is a significant risk factor for uterine fibroids, especially among women at the premenopausal stage and those ≥ 40 years of age. For instance, 60% of African American women aged 35-49 years reported uterine fibroids, whereas 80% of those aged ≥ 50 have uterine fibroids. Among White women, 40% of those aged ≤ 35 years and 70% aged ≥ 50 years developed uterine fibroids. Rapid growth of fibroids after the age of 30, especially in perimenoause, is consistent with age-related changes in oestrogen and progesterone. Fibroids have not been detected in prepubertal girls, and only sporadic cases have been reported in adolescents. However, the factor(s) involved in their development at such an early age is unknown. Due to the slight difference in biochemical pathways, uterine fibroids in young women do not exhibit typical uterine fibroid biology. In several cases, adolescent patients had a translocation between chromosomes 12 and 14, which is a confirmed risk factor for uterine fibroids. Women at the menopausal stage have shrunk uterine fibroid lesions and decreased sex hormones.
Early first period Women with an earlier age at menarche had higher levels of estradiol and estrone and lower levels of sex hormone-binding globulin than women with a later age at menarche.
Red meat? A diet higher in protein is protective however there has been a question mark around the risk of red meat increasing oestrogen. A study measuring the concentrations of oestrogen in American and Japanese beef found that the median concentrations of E2 and E1 in USA beef fat were 140 times and 11 times, respectively, higher than those in Japanese beef fat. In red meat, E2 and E1 levels of USA beef were ∼600 times and 10 times, respectively, higher than those of Japanese beef. It’s likely that the very high levels of E2 and E1 in American beef derive from the steroids given to the cattle. On the other hand, nearly zero level of E2 seen in Japanese beef was considered to be the natural endogenous status in beef without steroids. The go on to say “Accordingly, it is our intuitive feeling that the increasing consumption of oestrogen-rich beef following steroid implantation might facilitate oestrogen accumulation in the human body and could be related to the incidence of hormone-dependent cancers”, and very likely fibroids.
HRT A state-of-the-art literature review found that some combinations of oestrogen and progestin have exhibited a significant influence on fibroids enlargement, as well as in frequency of newly detected fibroids in menopause. By contrast, several studies failed to demonstrate a significant increase in fibroids size, although a trend towards enlargement was noted. Women should have regular thorough follow-up, including trans-vaginal ultrasound for the monitoring of fibroid size, and HRT should be discontinued if an increase in size of uterine fibroids is documented.
Obesity Fat tissue, has been proven to play hormonal, metabolic, and immune regulatory roles in the body. Fat cells make leptin, a hormone which in excess can promote inflammation driving fibroid growth. Additionally fat cells create a fibroid-friendly micro-environment that can induce fibrosis and fuel fibroid growth by increasing blood supply to it. Each kilogram of excessive body weight is correlated with an increased risk of uterine fibroids development. A study conducted in the United States found that women diagnosed with uterine fibroids are heavier than those without uterine fibroids. Moreover, an increase in the body mass index (BMI) by one unit, higher waist-to-hip ratios, and body fat percentage exceeding 30% increase the risk for uterine fibroids. Abdominal visceral fat also enhances this risk. Obesity and particularly excess visceral fat may be complemented with the reduced production of the sex hormone-binding globulin (SHBG), which binds circulating hormones, disrupting the hormonal activity toward sensitive tissues, and thereby influencing the delicate hormonal balance in the body.
Alcohol Alcohol and especially beer are known to increase oestrogen. A recent Korean study assessed alcohol consumption and the risk of new-onset fibroids in 2.5 million Korean women aged 20 to 39 years concluded:
Mild-to-Moderate Drinkers vs. Heavy Drinkers: Women who consumed alcohol had a higher chance of developing uterine leiomyomas. The increase in risk was between 12% and 16%. Specifically, women who drank alcohol mildly to moderately had about a 12% higher risk, while heavy drinkers had about a 16% higher risk.
Frequency of Drinking: The risk of developing these tumors increased with the frequency of alcohol consumption. Women who drank once a week had an 11% increased risk, while those who drank three or more times a week had a 15% increased risk.
Amount of Alcohol per Session: The risk also increased with the amount of alcohol consumed per session. Drinking seven or more glasses of alcohol in one session was associated with a 17% increased risk.
Sustained Drinkers vs. Sustained Non-Drinkers: Women who consistently consumed alcohol over a period of time (referred to as “sustained drinkers”) had a 20% increased risk of developing these tumors compared to women who consistently did not drink alcohol (referred to as “sustained nondrinkers”).
Change in Drinking Habits: Women who stopped drinking alcohol showed a small increase in risk (3%), whereas women who started drinking who previously did not have a 14% increased risk.
In summary, the study found that drinking alcohol is associated with a higher risk of developing uterine leiomyomas, and this risk increases with the amount and frequency of alcohol consumption. Women who consistently drink have a notably higher risk compared to those who don’t drink or those who stopped drinking.
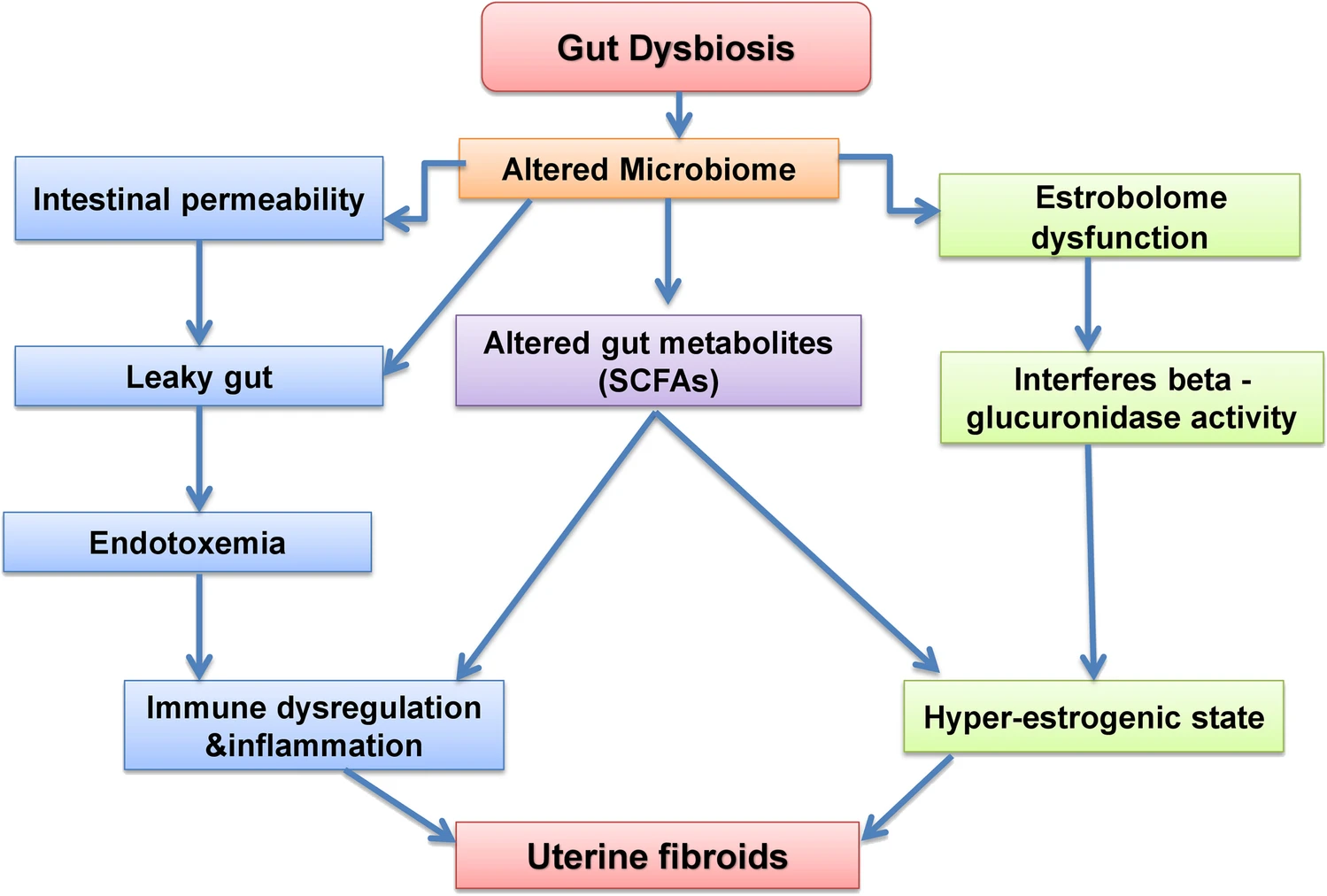
An imbalanced gut microbiome The estrobolome is a collection of bacteria in the gut which is capable of metabolising and modulating the body’s circulating oestrogen. The gut bacteria regulate oestrogens through secretion of β-glucuronidase, an enzyme that splits detoxified oestrogen, releasing free oestrogens that are then reabsorbed into the bloodstream and repeatedly circulated through the body, increasing oestrogen levels. The genes for β-glucuronidase are widely found in Firmicutes (which are increased in the vaginal microbiome in women with fibroids, see below).
A dysbiotic gut results in an altered microbiome which triggers the following pathways
interferes with the estrobolome functioning and results in hyperestrogenic state leading to uterine fibroids
altered levels of gut metabolites such as short chain fatty acids (SCFA) which triggers immune dysregulation and induce inflammation and also leads to hyperestrogenic state
interferes the gut permeability leading to a leaky gut and toxicity which could dysregulate the immune function.
COMT Catechol-O-methyltransferase (COMT) is an enzyme that triggers enhanced transformation of 2-hydroxyestradiol (anti-estrogen) into 2-methoxyestradiol (pro-estrogen) with resultant hyperestrogenic environment that may contribute to cell proliferation and increase in fibroid development. High COMT activity has been found in fibroids. Women with the high-activity COMT Val/Val genotype are 2.5 times more likely to develop fibroids than women with other genotypes. The prevalence of this genotype was significantly higher in African American women (47%) compared with white (19%) or Hispanic (30%) women.
MTFHR Methylenetetrahydrofolate reductase (MTHFR) plays a key role in the enzymatic process in the folate metabolism pathway, which converts folic acid (obtained from food and/or supplements) into methyl-folate (the form of folate used by your body), and then participates in DNA synthesis, modification and methylation. The mutation of the MTHFR C677T gene leads to the disorder of folate metabolism, the decrease of antioxidant capacity, the increase of uterine related oxidative stress, and the proliferation of uterine smooth muscle cells, thus leading to the formation of fibroids. Additionally MTHFR mutations can cause high blood pressure via increased homocysteine. Vitamin B2 (riboflavin) is a required cofactor for MTFHR and higher vitamin B2 levels are associated with increased MTHFR enzyme activity, lower homocysteine and improved blood pressure.
Genetic testing has identified:
The wildtype (non-variant) MTHFR 677 shown as “CC”. This is associated with 100% enzyme activity and does not increase risk for higher homocysteine or high blood pressure.
A single MTHFR 677 variation shown as “CT”. This results in 30-35% reduction in enzyme activity and can slightly increase risk for higher homocysteine levels and blood pressure.
A double MTHFR 677 variation shown as “TT”. This results in 60-70% reduction in enzyme activity and increases the risk for higher homocysteine and high blood pressure.
A study this year reported that women with untreated hypertension faced an 18% higher risk of developing uterine fibroids when compared to those without hypertension. Conversely, women with hypertension who were using blood pressure medications had a 37% lower risk of developing uterine fibroids, with the use of angiotensin-converting enzyme inhibitors associated with a 48% lower risk. Interestingly, women with new-onset hypertension had a 45% greater risk of uterine fibroid diagnosis, while those with pre-existing hypertension had little additional risk. The formation of fibroids is attributed to the chronic destruction of the uterine lining due to increased blood flow and inflammation.
Vitamin D deficiency
A systematic review last year concluded that 100% of all research studies identified vitamin D deficiency in women with uterine fibroids. The best estimate of the effect of hypovitaminosis D on fibroid development found that deficient vitamin D (< 20 ng/mL) increased the risk of uterine fibroids by 32%. The importance of this relationship is underscored by the prevalence of vitamin D deficiency, a condition which affects approximately 80% of Black American women, a population disproportionately affected by fibroids.
Women at risk for deficiency should be screened and those with deficiency should take supplements. The functional range for vitamin D is 125-150. I usually recommend 10,000 IU a day at deficiency below 60 and test serum levels regularly to avoid any overdose-related toxicities. Routine vitamin D supplementation for women with insufficiency may provide effective treatment and prevention of fibroids.
Imbalanced vaginal microbiome
A recent study showed that an increased level of the bacterial phyla Firmicutes was observed in both the cervical and vaginal microbiome of women with fibroids. An increased level of Firmicutes is associated with obesity. Firmicutes include Lactobacillus, Streptococcus, Clostridia, and can be reduced with high animal protein diet.
Uterine infections
Fibroids are associated with Chlamydial infection, and pelvic inflammatory disease. The risk of fibroids is increased 5x when infections are associated with the copper coil.
Copper Intrauterine Devices (IUD)
The copper coil may be a cause of uterine fibroids. Intrauterine devices can cause local irritation, pressure, inflammation, and tissue changes in the uterus. Copper IUDs in particular impact cellular mechanisms in the endometrium. There may be oedema, vascular congestion, cell death, and other cytological alterations. These effects involve inflammatory cytokines and changes in cell proliferation and activity that have been associated with fibroids: Interleukin 1 beta (IL-1β) and tumour necrosis factor-alpha (TNF-α) levels were high in the late secretory phase and IL-6 levels were high in the proliferative early secretory phase in IUD-subjected endometrial samples. The expression of IL-1, IL-6, and TNF-α was found to be associated with the pathophysiology of uterine fibroids. A study concluded that the use of copper IUDs for more than 2 consecutive years should be avoided in order to prevent oxidative damage.
Copper T380A is one of the most commonly prescribed IUDs and has been shown to significantly increase copper levels. The use of copper T-200 IUD for 12 months significantly increased copper levels and significantly decreased zinc and iron levels. It is suggested that the low zinc status was probably responsible for the heavy bleeding which was common among the study group using copper IUDs, which in turn was responsible for the anaemia seen in more than 50% of the IUD users.
The adverse effects of copper intrauterine devices (IUDs) such as abnormal bleeding, pain and cramps may be due in part to the burst release of copper ions during the first few months of usage. Copper can then continue to build up slowly in the body. Coppertoxic.com reports: “For many women, symptoms often first begin appearing 2 or 6 months after insertion. For others, the time period may be much longer, years to decades, before they notice anything, or connect the dots. Side effects of the copper IUD as copper accumulates usually begin with increasing brain fog and fatigue, often paired with a racing mind. Eventually, once the liver is overloaded, copper will then start accumulating more in the brain, and severe shifts in personality can occur as a result of increasing bio-unavailable copper and calcium and changes in neurotransmitter production. The period 2 to 5 months post-insertion is a common time for many women when metabolism begins slowing and energy, behaviour, and reactions begin changing, especially with a tendency towards increasing depression and irritability.”
Estrogen is known to increase copper absorption vice versa. Having an excess of copper in the body has been linked to being one of the key underlying drivers of anxiety, oestrogen dominance, painful periods, heavy periods, irregular periods, mental health issues, and overall hormonal imbalances.
Toxic pollutants
Common chemicals called phthalates found in hundreds of household products have been linked to fibroids. Phthalates are present in many household items ranging from food packaging and processing equipment to shower curtains, building materials, and car interiors. Phthalates are also used as solvents in cosmetics and other personal care products and to coat or encapsulate certain pharmaceutical pills and dietary supplements. The chemicals can leach out of these products and enter food, air, and water, meaning you can swallow, inhale, or absorb these phthalate particles through direct skin contact. The body then metabolises these chemicals, yielding byproducts that several studies have detected in human urine, breastmilk, and blood.
A systematic review and application of social, structural, and political context to racial disparities in uterine fibroids found that Black women face worse clinical and surgical outcomes than their white counterparts. The differences in gene expression in fibroids from Black and white women, as well as racial disparities in fibroid prevalence, they say, may reflect that Black individuals disproportionately experience exposures linked with increased risk for uterine fibroids.
This includes a higher risk of chronic psychological stress, adverse childhood experiences, perceived racism and environmental contaminant exposures like air pollution among Black women, which have all been associated with a higher risk for developing and experiencing severe symptoms from fibroids.
Racial disparities may also stem from other social determinants of health such as a higher fat diet, lower levels of physical activity, vitamin D deficiency, as well as individual behaviours such as use of chemical hair relaxers that contain chemicals that are associated with increased risk of uterine fibroids. Studies have also suggested racial disparities in uterine fibroids and endometriosis can be linked to a lack of adequate access to health care, authors note, including minimally invasive gynecologic surgeons, interventional radiologists, and bias and discrimination within the health care system. “Black women may be more likely to have symptoms dismissed, report negative experiences with the health care system and wait too long to see a specialist, which delays diagnosis and treatment,” the author said. “These significant differences in experiences, access and dismissal or misattribution of symptoms may lead to worse outcomes.”
While some women with fibroids don’t have symptoms, others have significant pain, anaemia, heavy menstrual bleeding, increased urinary frequency, fertility problems and pregnancy complications. Black women are diagnosed with fibroids roughly three times as frequently as white women, develop them earlier in life and tend to experience larger and more numerous fibroids that cause more severe symptoms. The author of the study said “If we are sincere about striving for health equity, then we have to look at the underpinnings of inequity in our healthcare system and in society. Solutions need to address root causes of disparities through policy, education and programs that ensure all patients receive competent care.”
6. Associations
Association with Breast Lumps (fibroadenoma)
The same mutated MED12 gene that is found to cause fibroids is also found in 59% of breast fibroadenomas. This indicates that benign tumours of the breast and uterus, both of which are key target tissues of oestrogen, may share a common genetic basis underpinned by highly frequent and specific MED12 mutations. Interestingly supplementing with iodine resolves breast lumps and breast pain which may indicate that iodine deficiency is also a driver for fibroid development.
Tissues that store iodine include the thyroid, breasts, ovaries, uterus and placenta. While the thyroid tends to concentrate a higher percentage of iodide (I¯), other tissues tend to utilise a greater percentage of molecular iodine (I₂), which exerts multiple and complex actions related to its role as an antioxidant, an anti-inflammatory, a pro-inflammatory, an inducer of cell death, an immune modulator, and a promotor of cell differentiation. Importantly, iodine helps to maintain the oestrogen balance in favour of estriol which has been shown to protect against oestrogenic cancers and decrease the risk of fibrocystic changes in the breasts.
High oestrogen levels can prevent the absorption of iodine, which may be an additional cause of fibroid development. Iodine deficiency has been associated with fibrocystic breast disease and, more recently, with the development of distant metastatic breast cancer in young women aged 25-39. This trend toward the development of breast cancer in younger women has been associated with the reemergence of iodine deficiency in the U.S. since the 1970s. Since iodine protects against abnormal cell development and proliferation, adequate iodine levels may prevent fibroids from occurring.
Women with fibroids should be more vigilant about breast cancer, having regular breast exams and ultrasound for early detection of breast cancer.
7. Advances in Surgical Treatment
Traditional surgical treatments for fibroids are:
Removing the whole womb including the fibroids (a hysterectomy). This is an option for women who do not want to have any (more) children.
Removing the fibroids only (called myomectomy). This type of operation is suitable for women who want to keep their uterus – mainly to preserve the chance for future pregnancy.
More recent surgical treatments for fibroids include:
Removing the fibroid through keyhole surgery (laparoscopic myomectomy).
Blocking the blood vessels feeding the fibroids (uterine artery embolization) which does not remove fibroids but can cause them to shrink and reduce heavy periods.
Some fibroids that are growing inside the the womb can be removed through a hysteroscope passed inside the womb through the cervix.
There are many factors to consider when deciding the best way of removing fibroids. These include the number of fibroids, their size and exactly where they are in the womb. There can also be other issues to consider like whether you have had any operations on the womb in the past. For example, some of the fibroids that grow inside the womb can be removed by using hysteroscope operations. The fibroids that are more embedded in the womb itself cannot be removed this way.
In the last few years some hospitals have been offering SONATA: Sonography-Guided Transcervical Fibroid Ablation. It is an incisionless, uterus-preserving, transcervical approach, with real-time visualisation using intrauterine ultrasound guidance, and combines ultrasound imaging with radiofrequency energy.
Recently scientists have been developing a new therapeutic treatment using a drug capable of breaking fibroids down inside the body. Since fibroids are collagen-based, the key ingredient in this intervention is collagenase, an enzyme that digests collagen, and it is combined with LiquoGel™, which is liquid at room temperature, and becomes a gel at body temperature. Because of that, once it gets injected into a fibroid, it becomes a gel. Over time, collagenase will degrade the fibroid and LiquoGel™ will degrade, allowing the body to get rid of it. Much work remains before the treatment can reach patients.
8. Tests to Consider for Evaluation Fibroids
Transvaginal and abdominal ultrasonography
To determine the size and location of fibroids and rule out ovarian tumors
Progesterone/estradiol ratio (100–300:1) Luteal phase progesterone measurement
Low luteal phase progesterone level support oestrogen dominance and fibroid growth
Vitamin D test
Low levels increase fibroid growth by several mechanisms
Vitamin A test
Low levels shown to increase heavy bleeding
Iron or total iron-binding capacity measurement, ferritin tests
Low iron stores reduce uterine contractions and increase menstrual blood loss
Zinc and copper tests
An imbalanced copper:zinc ratio can lead to fibroids
Thyroid function testing
Hypothyroidism associated with menstrual dysfunction
MTFHR testing
35% weakness in methylation, increased oestrogen dominance
DUTCH testing for Phase 1 and Phase 2 oestrogen detoxification evaluation
Unhealthy oestrogen metabolism contributes to oestrogen dominance
Comprehensive digestive stool analysis
Intestinal dysbiosis is a cause of oestrogen dominance through several mechanisms
Vaginal microbiome testing
An unbalanced vaginal microbiome has been associated with fibroids
Testing for celiac disease (antigliadin antibodies)
Gluten grain sensitivity common in fibroid sufferers and can lead to further oestrogen dominance
9. My approach to treating fibroids
My personal experience with fibroids, and supporting women with fibroids, clearly shows that nutrition, supplements and lifestyle changes can make a significant impact on fibroid size, heavy bleeding and pain to the point of not creating any symptoms. I initially ask clients to commit to a 3-month trial period, during which they will do as much of their protocol as possible. At the end of these first 3 months, we assess symptoms, such as heavy bleeding and pain, and any growth or shrinkage of the fibroids. The protocol is considered successful if the client perceives a reduction in symptoms and no further fibroid growth has occurred. We then continue the program for 3-month periods while continuing to monitor symptoms and uterine size. If at any time symptoms recur or worsen or the fibroids begin to grow, other more aggressive measures must be considered.
Nutrition
Women with fibroids begin a hormone-balancing diet involving foods with low inflammation effects, low acidity, and a low glycemic load.
Reduce foods that increase oestrogen dominance:
Foods that are acidic and inflammatory, like red meat, poultry, and dairy, contain arachidonic acid. This acid can increase inflammation and help fibroids grow. Avoiding commercial meat products also reduces exposure to added hormones. Small amounts of range-fed meats can be added back once inflammation goes down.
Sweets and high glycemic foods can cause stress and raise insulin. This can increase oestrogen dominance and help fibroids grow. Eating breakfast with protein, fat and quality carbs prevents drops in blood sugar. This avoids spikes in cortisol and adrenaline, which break down muscle and raise insulin resistance.
Gluten grains like wheat, rye and barley contain a strong gluten that is genetically engineered. This gluten can raise oestrogen by blocking the detoxifying cytochrome P450 3A4 enzyme system. It can also affect thyroid hormones. Anyone with high oestrogen should be tested for gluten sensitivity.
Alcohol, dairy, coffee, artificial ingredients, colours, flavours and preservatives should be avoided. Also avoid margarines and foods with trans fats or hydrogenated oils.
Include foods that reduce oestrogen dominance:
Cruciferous vegetables such as broccoli, Brussels sprouts, cabbage, and cauliflower support healthy oestrogen metabolism.
3 cups of green tea daily are helpful (to reduce COMT activity).
Gut and Vaginal Microbiome Restoration, and Detoxification
Healing intestinal and vaginal microbiome imbalance and supporting liver detoxification restores hormone balance and remove sources of inflammation.
Supplements
These nutrients to support hormone metabolism and reduce inflammation:
Vitamin B complex, methylated
Vitamin D
Vitamin A
Indole-3-carbinol or diindolylmethane (DIM) to reduce estrogen dominance
Aromatase inhibitors such as Myomin can reduce oestrogen dominance
Calcium D glucarate can reduce increased recirculation of oestrogens from the gut back into the body
Iodine
Calcium: significant negative associations have been found between low serum calcium levels and uterine fibroids, uterine size and the number of fibroid nodules, possibly reflecting associated low vitamin D levels
Selenium has been shown to reduce fibroid size, possibly because it is an integral part of the antioxidant enzymes glutathioneperoxidase, catalase, and superoxide dismutase (SOD) which neutralise oxidative toxic intermediates, and of which there is a deficiency in fibroids.
Chronic insomnia disorder is one of the most common problems in postmenopausal women, exacerbated by underdiagnosis and improper treatment.
This double-blinded, randomized, placebo-controlled trial was conducted to evaluate the potential of vitamin E to treat chronic insomnia as an alternative to sedative drugs and hormonal therapy.
The study enrolled 160 postmenopausal women with chronic insomnia disorder, divided randomly into two groups. The vitamin E group received 400 units of mixed tocopherol daily, while the placebo group received an identical oral capsule.
The primary outcome of this study was sleep quality assessed by the Pittsburgh Sleep Quality Index (PSQI), a self-evaluated and standardized questionnaire. The secondary outcome was the percentage of participants using sedative drugs. There were no significant differences in baseline characteristics between the study groups. However, the median PSQI score at baseline was slightly higher in the vitamin E group compared with the placebo. After one month of intervention, the PSQI score was significantly lower (indicating better sleep quality) in the vitamin E group compared with the placebo.
Moreover, the improvement score was significantly higher in the vitamin E group compared with the placebo. In addition, there was a significant reduction in the percentage of patients using sedative drugs in the vitamin E group (15%), while this reduction was not statistically significant in the placebo group (7.5%).
This study demonstrates vitamin E’s potential as an excellent alternative treatment for chronic insomnia disorder that improves sleep quality and reduces sedative drug use.
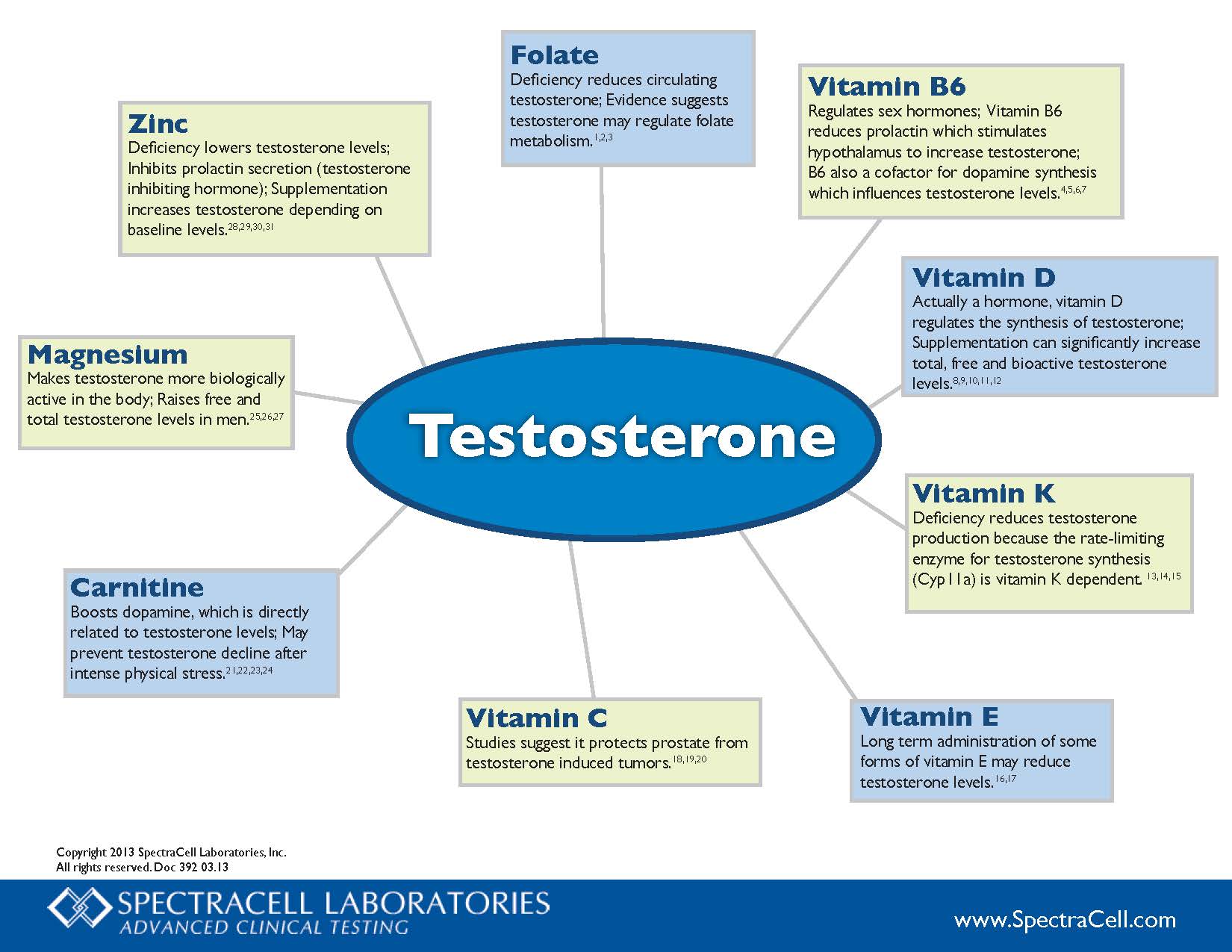
Vitamin B6 Regulates sex hormones; Vitamin B6 reduces prolactin which stimulates hypothalamus to increase testosterone; B6 also a cofactor for dopamine synthesis which influences testosterone levels.4,5,6,7
Vitamin D Actually a hormone, vitamin D regulates the synthesis of testosterone; Supplementation can significantly increase total, free and bioactive testosterone levels. 8,9,10,11,12
Vitamin K Deficiency reduces testosterone production because the rate-limiting enzyme for testosterone synthesis (Cyp11a) is vitamin K dependent. 13,14,15
Vitamin E Long term administration of some forms of vitamin E may reduce testosterone levels.16,17
Vitamin C Studies suggest it protects prostate from testosterone induced tumors.18,19,20
Carnitine Boosts dopamine, which is directly related to testosterone levels; May prevent testosterone decline after intense physical stress.21,22,23,24
Magnesium Makes testosterone more biologically active in the body; Raises free and total testosterone levels in men.25,26,27
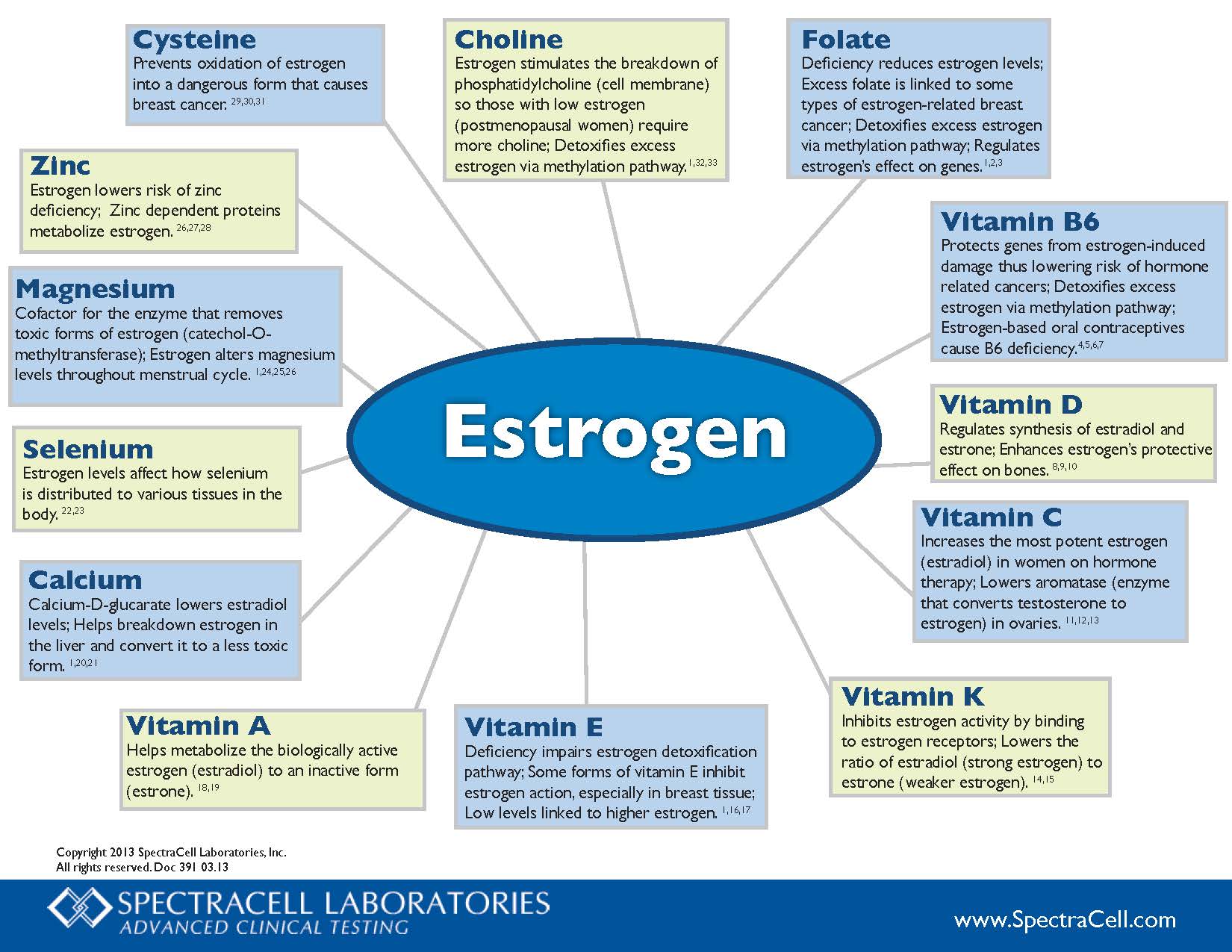
Choline – Estrogen stimulates the breakdown of phosphatidylcholine (cell membrane) so those with low estrogen (postmenopausal women) require more choline; Detoxifies excess estrogen via methylation pathway.1,32,33
Folate – Deficiency reduces estrogen levels; Excess folate is linked to some types of estrogen-related breast cancer; Detoxifies excess estrogen via methylation pathway; Regulates estrogen’s effect on genes.1,2,3
Vitamin B6 – Protects genes from estrogen-induced damage thus lowering risk of hormone related cancers; Detoxifies excess estrogen via methylation pathway; Estrogen-based oral contraceptives cause B6 deficiency.4,5,6,7
Vitamin D – Regulates synthesis of estradiol and estrone; Enhances estrogen’s protective effect on bones.8,9,10
Vitamin C – Increases the most potent estrogen (estradiol) in women on hormone therapy; Lowers aromatase (enzyme that converts testosterone to estrogen) in ovaries.11.12.13
Vitamin K – Inhibits estrogen activity by binding to estrogen receptors; Lowers the ratio of estradiol (strong estrogen) to estrone (weaker estrogen).14,15
Vitamin E – Deficiency impairs estrogen detoxification pathway; Some forms of vitamin E inhibit estrogen action, especially in breast tissue; Low levels linked to higher estrogen.1,16,17
Vitamin A – Helps metabolize the biologically active estrogen (estradiol) to an inactive form (estrone).18,19
Calcium – Calcium-D-glucarate lowers estradiol levels; Helps breakdown estrogen in the liver and convert it to a less toxic form.1,20,21
Selenium – Estrogen levels affect how selenium is distributed to various tissues in the body.22,23
Magnesium – Cofactor for the enzyme that removes toxic forms of estrogen (catechol-O-methyltransferase); Estrogen alters magnesium levels throughout menstrual cycle.1,24,25,26
Menopause is associated with increased risks for cardiovascular disease, osteoporosis, and cancer. Many women experience declining energy, mood, cognitive function and memory during menopause.
Rhodiola rosea extracts have been shown to enhance mood, cognitive function, and memory. Moreover, these extracts possess anti-stress, neuroprotective, cardiovascular-protective, and anticarcinogenic properties, which are particularly valuable to counteract some of the common health risks seen in women as they age. R. rosea is low in side effects compared to synthetic selective estrogen receptor modulators (SERMS).
Preclinical and clinical studies suggest that R. rosea extracts provide a combination of effects that could counteract the adverse consequences of estrogen decline by improving neurological, endothelial, and cardiovascular functions.
As a natural SERM, R. rosea could alleviate menopause-related symptoms while conferring additional neuro-protective, cardio-protective, anti-stress, anti-fatigue, osteoprotective, and other health benefits.
Unlike HRT, preliminary evidence indicates that orally ingested R. rosea extracts are unlikely to cause estrogenic effects or increased the risk of cancer in hormone sensitive tissues. R. rosea extracts and salidroside do not significantly stimulate, but rather inhibit growth of human breast cancer in vitro and in vivo in some studies. Human studies are needed to verify the safety of R. rosea in postmenopausal women who are at increased risk or who are being treated for breast cancer.
Further research on the use of R. rosea alone and in combination with other adaptogens during menopause would enable development of this promising alternative SERM.
Endometriosis is a chronic gynecologic disease process with multifactorial etiology. Increased oxidative stress, a result of increased production of free radicals or depletion of the body’s endogenous antioxidant defense, has been implicated in its pathogenesis. Oxidative stress is thought to promote angiogenesis and the growth and proliferation of endometriotic implants. Oxidative stress in the reproductive [...]
Endometriosis is a chronic gynecologic disease process with multifactorial etiology. Increased oxidative stress, a result of increased production of free radicals or depletion of the body’s endogenous antioxidant defense, has been implicated in its pathogenesis. Oxidative stress is thought to promote angiogenesis and the growth and proliferation of endometriotic implants. Oxidative stress in the reproductive tract microenvironment is known to negatively affect sperm count and quality and may also arrest fertilized egg division leading to embryo death. Increased DNA damage in sperm, oocytes, and resultant embryos may account for the increase in miscarriages and fertilization and implantation failures seen in patients with endometriosis.
The evidence linking endometriosis and infertility to endogenous pro-oxidant imbalance provides a rationale for the empiric use of antioxidant therapy. Vitamin C and E deficiency has been demonstrated in women with endometriosis. Observational and randomized controlled studies have shown vitamin C and E combination therapy to decrease markers of oxidative stress.
Endometriosis is a chronic gynecologic disease process with multifactorial etiology. Increased oxidative stress, a result of increased production of free radicals or depletion of the body’s endogenous antioxidant defense, has been implicated in its pathogenesis. Oxidative stress is thought to promote angiogenesis and the growth and proliferation of endometriotic implants. Oxidative stress in the reproductive tract microenvironment is known to negatively affect sperm count and quality and may also arrest fertilized egg division leading to embryo death. Increased DNA damage in sperm, oocytes, and resultant embryos may account for the increase in miscarriages and fertilization and implantation failures seen in patients with endometriosis.
The evidence linking endometriosis and infertility to endogenous pro-oxidant imbalance provides a rationale for the empiric use of antioxidant therapy. Vitamin C and E deficiency has been demonstrated in women with endometriosis. Observational and randomized controlled studies have shown vitamin C and E combination therapy to decrease markers of oxidative stress.
Endometriosis is a painful condition of the female reproductive organs that can result in heavy bleeding, scarring, fatigue, infertility, and more.
A study published in April 2018 using data collected from 70,835 premenopausal women has examined if there is a connection between fruit and vegetable consumption and endometriosis. While there didn’t appear to be an association between total vegetable intake and risk of endometriosis, citrus fruits were associated with a lower risk of the disease. Based on data from food frequency questionnaires every four years between 1991 to 2013, women consuming ≥1 servings of citrus fruits per day had a 22% lower endometriosis risk compared to those consuming <1 serving per week.
The researchers concluded, “Our findings suggest that a higher intake of fruits, particularly citrus fruits, is associated with a lower risk of endometriosis, and beta-cryptoxanthin in these foods may partially explain this association.”
As search for optimal therapy continues for endometriosis, aid of dietary supplements is gaining attention. Supplements can be used for their anti-inflammatory, anti-oxidant, anti-proliferative and immune modulatory characteristics. We reviewed the literature, evaluated and synthesized effects of vitamin D, zinc, magnesium, omega 3, propolis, quercetin, curcumin, N-acetylcysteine, probiotics, resveratrol, alpha lipoic acid, vitamin C, vitamin E, selenium and epigallocatechin-3-gallate. Based on results of in vitro, animal and human studies, it might be safe to say that dietary supplements can be used as a complementary treatment for endometriosis.
To prove the efficacy of oral vitamin B1 administration for the treatment of primary dysmenorrhoea, a randomised, double-blind, placebo-controlled study was carried out on 556 girls aged 12-21 yr, having moderate to very severe spasmodic dysmenorrhoea.
Thiamine hydrochloride (vitamin B1) was given in a dose of 100 mg orally, daily for 90 days.
The combined final results of both the ‘active treatment first’ group and the ‘placebo first’ group, after 90 days of vitamin B1 administration, were
87 per cent completely cured,
8 per cent relieved (pain almost nil to reduced)
5 per cent showed no effect whatsoever.
The results remained the same two months later as well when no drug was administered. Unlike all the current treatments which are suppression-oriented, this curative treatment directly treats the cause, is free from side effects, is inexpensive and easy to administer.
Endometriosis is a common chronic inflammation causing major problems including infertility. The role of omega-3 and omega-6 fatty acids as their potential anti-inflammatory effects in endometriosis needs to be further explored. The objective of this study was to compare serum phospholipid fatty acid profile in endometriosis patients with controls, and to explore the correlation of this profile with the severity of the disease.
Methods:
Sixty-four endometriosis patients and 74 control women, in reproductive age, participated in this study. Among the endometriosis patients, 19 cases were in stage I, 27 cases in stage II, 8 cases in stage III, and 10 cases in stage IV. Each patient underwent laparoscopy. Before surgery, 5 ml of blood was obtained. After extraction of the total lipids, serum total phospholipid fraction was isolated by thin layer chromatography. Fatty acid composition of the phospholipid fraction was determined by gas chromatography and the resulted profile was compared in endometriosis patients and controls. The profile was also compared in the endometriosis group based on the severity of disease.
Results:
Stearic acid was significantly lower in the endometriosis group as compared to controls (P= 0.030). No other fatty acid compositions were significantly different between patients and controls. Serum ratio of eicosapentaenoic acid (EPA) to arachidonic acid (AA) was in reasonable correlation with the severity of endometriosis (r = 0.34, P = 0.006).
Conclusion:
According to these findings, levels of fatty acids in serum total phospholipids seem not to be a marker for endometriosis, but the EPA to AA ratio was a relevant factor indicating severity of illness.
EPA is hypothesized to reduce disease severity through their anti-inflammatory and immunomodulatory effects [25]. EPA is the most important component of omega-3 and AA, an omega-6 fatty acid and plays an important role in biological systems. AA has a substrate role for production of certain mediators such as PGE2 and leukotriene (LTB4). PGE2 and LTB4 are initiators for endometriosis and pain [24]. On the other hand, EPA plays a role in biosynthesis of LTB5 and PGE3 which have less inflammatory effect compared with PGE2 and LTB4 [24]. EPA is a competitive inhibitor in conversion of AA to LTB4 and PGE2 [26]. Irrespective of study design, our results were in agreement, in part, with the in vitro experiments by Gazvani et al. [20] that showed a high ratio of omega-3 to omega-6 in endometrial cell culture from endometriosis patients induce higher concentrations of IL-8 productions in cell supernatant. IL-8 as a pro-inflammatory and angiogenic cytokine has a significant role in endometriosis [27].
Infertility affects as many as 12.3% of women ages 15-44 (or 7.5 million women) in the United States.
Consequently, it is imperative to find methods to help women overcome infertility so that they may conceive a healthy child.
Many of the current treatments for infertility are costly, have low success rates, and have the potential to negatively affect long-term health. The common medical interventions used for infertility include fertility medications, in-vitro fertilization (IVF), and intrauterine insemination (IUI). Fertility medications, such as clomiphene and gonadotropins, stimulate growth of the ovarian follicle, followed by follicular rupture induced by a human chorionic gonadotropin (hCG) trigger shot.
These medications are often used in conjunction with IVF and IUI. IVF is an assisted reproductive technology that includes combining an egg and a sperm in a laboratory and then transferring the fertilized embryo into the uterus. IUI involves placing the sperm inside of the uterus to help with fertilization. Although less invasive and expensive than IVF, in IUI the sperm has to fertilize the egg on its own within the woman’s reproductive tract.
Research suggests a link between a variety of health conditions and subsequent infertility, including polycystic ovarian syndrome (PCOS), endometriosis, advanced maternal age (AMA), high body mass index (BMI), the MTHFR genetic mutation, hypothyroidism (both clinical and subclinical), and poor ovarian reserve.
In this article, we provide case evidence for alternative methods for managing infertility that are effective at improving the underlying condition leading to infertility – methods that are less expensive than medical intervention and are supportive of long-term health.
NAC (N-acetylcysteine) treatment or no treatment was offered to 92 consecutive Italian women referred to our university hospital with ultrasound confirmed diagnosis of ovarian endometriosis and scheduled to undergo laparoscopy 3 months later.
According to patients acceptance or refusal, NAC-treated and untreated groups finally comprised 73 and 72 endometriomas, respectively.
After 3 months, within NAC-treated patients cyst mean diameter was slightly reduced (−1.5 mm) versus a significant increase (+6.6 mm) in untreated patients (P = 0.001).
Particularly, during NAC treatment, more cysts reduced and fewer cysts increased their size.
Our results are better than those reported after hormonal treatments.
Twenty-four NAC-treated patients—versus 1 within controls—cancelled scheduled laparoscopy due to cysts decrease/disappearance and/or relevant pain reduction (21 cases) or pregnancy (1 case).
Eight pregnancies occurred in NAC-treated patients and 6 in untreated patients.
We can conclude that NAC actually represents a simple effective treatment for endometriosis, without side effects, and a suitable approach for women desiring a pregnancy
Supplementation with myo-inositol may be considered a reliable option in the treatment of metabolic syndrome in postmenopausal women.
The aim of this study was to evaluate whether myo-inositol, an insulin-sensitizing substance, may improve some features of metabolic syndrome in postmenopausal women.
Methods:
Eighty postmenopausal women affected by the metabolic syndrome were enrolled prospectively in the study and treated with diet plus supplementation of myo-inositol (2 g BID plus diet: intervention group) or with diet plus placebo (control group) for 6 months. They were evaluated at baseline and after 6 months for insulin resistance (homeostasis model assessment ratio [HOMA] insulin resistance), lipid profile, and blood pressure.
Results:
Myo-inositol plus diet improved systolic and diastolic blood pressure, HOMA index, cholesterol, and triglyceride serum levels with highly significant differences, compared with the groups treated only with diet and placebo. In the group treated with myo-inositol, a decrease in diastolic blood pressure (−11%), HOMA index (−75%), and serum triglycerides (−20%) and an improvement in high-density lipoprotein cholesterol (22%) were shown.
Conclusions:
Supplementation with myo-inositol may be considered a reliable option in the treatment of metabolic syndrome in postmenopausal women.
Polycystic ovary syndrome (PCOS) is a complex and common endocrine disorder characterized by hyperandrogenism, which is accompanied by follicle growth arrest at the small antral stage, minimal granulosa cell proliferation, and chronic anovulation.
Polyunsaturated fatty acids (PUFAs) are necessary for the body’s metabolism, growth and development. Although PUFAs play an important role in the regulation of female reproduction, their role in ovarian development in PCOS is still unclear.
The present study was conducted to investigate the effects of different ratios of n-3/n-6 PUFAs (omega-3/omega-6) on ovary development in PCOS rats. Serum levels of reproductive hormones and enzymes related to steroidogenesis were assessed.
The results indicated that PUFAs (n-3/n-6: 1/15) significantly increased ovarian weight and improved the ovarian structure although they had no significant effect on body weight in PCOS rats.
Meanwhile, apoptosis was attenuated accompanied by increased cell proliferation by PUFAs (n-3/n-6: 1/15). Moreover, serum levels of hormones (FSH and E2) were also significantly increased by PUFAs (n-3/n-6: 1/15) accompanied by decreased T levels.
To investigate whether PUFAs regulate the expression of enzymes related to hormone synthesis, western blotting was used to determine the protein levels of CYP51, CYP19, StAR and 3β-HSD.
The results showed that PUFAs significantly increased the protein levels of all of these enzymes. These results indicate that PUFAs enhance the reproductive performance of PCOS by increasing the expression of steroidogenesis enzymes, which are related to hormone secretion and ovarian functions.
These findings provide evidence that a balanced n-3/n-6 PUFA ratio is beneficial for PCOS reproduction.
There is now compelling evidence for a link between enteric microbiota and brain function. The ingestion of probiotics modulates the processing of information that is strongly linked to anxiety and depression, and influences the neuroendocrine stress response.
This study found that taking a prebiotic called galactooligosaccharides for three weeks significantly reduced the amount of cortisol, a primary stress hormone in the body.
Fibroids – uterine leiomyomas (ULMs) – are estrogen-dependent tumors that are more common in African American women. The aetiology for such ethnic disparity is currently unknown. Catechol-O-methyltransferase (COMT) is an essential enzyme in estrogen metabolism.
Women with the high-activity COMT genotype are 2.5 times more likely to develop ULMs than women with other genotypes. The prevalence of this genotype was significantly higher in African American women (47%) compared with white (19%) or Hispanic (30%) women. Myometrial cell lines expressing the Val/Val genotype exhibited significantly enhanced responses to estrogen in proliferation and in estrogen-responsive element reporter assays. COMT-specific inhibitors reversed such a response and induced apoptosis. Myometrial specimens from Val/Val women demonstrated distinct estrogen-regulated gene expression that was consistent with enhanced proliferation and decreased apoptosis.
The results provide a possible explanation for the higher prevalence of ULMs among African American women and offer a potential new target for nonsurgical treatment using COMT inhibitors.
Metabolic syndrome is a cluster of conditions that occur together, including
increased blood pressure
high blood sugar
excess body fat around the waist, and
abnormal cholesterol or triglyceride levels.
Having just one of these conditions doesn’t mean you have metabolic syndrome but as you develop more of these conditions, your risk of complications such as type 2 diabetes and heart disease, rises higher and higher.
Research shows that the more carbohydrates you eat, the more likely you are to have metabolic syndrome:
for every 5% intake of energy from carbohydrates, the increase in the risk of metabolic syndrome goes up by 2.6%.
We tend to think that a loss of mental acuity is just part of getting older — but age is not the only contributing factor to cognitive decline. Our lifestyle also plays a key role. Failing to follow a nutritious diet, a lack of sleep and exercise, ongoing stress, smoking, drinking alcohol excessively and environmental pollutants can all damage our brain cells.
Fortunately, mental deterioration is not irreversible. In fact, the brain is incredibly dynamic and has the potential and the ability to change at any point throughout our entire life – and you have the power to enhance your brain function, protect your brain from damage and counteract the effects of aging! That is, if you’re willing to fuel the brain and tweak your everyday decisions.
Here are 5 small changes you can make in your life that can mean big differences in your cognitive abilities.
As women start to produce less estrogen and enter perimenopause, they are likely to experience a mix of challenging symptoms. These include hot flashes, insomnia, night sweats, vaginal dryness, and mood swings.
Menstrual periods may get lighter or heavier and less regular, but once a woman has not had a period for 12 months, they are in menopause. Then, the symptoms experienced over the previous years begin to subside.
There is a range of vitamins and supplements available to help women manage the symptoms of perimenopause and menopause.
If you feel as though you can’t do as much physically as you’ve gotten older, there may be a reason. Both aging and menopause are known to affect sarcopenia, which is a loss of muscle mass and strength, which in turn affects balance, gait, and overall ability to perform tasks of daily living. A new study is one of the first to link alcohol consumption with a higher prevalence of sarcopenia in postmenopausal women. The study outcomes are being published online today in Menopause, the journal of The North American Menopause Society (NAMS).
Previous studies of postmenopausal women have suggested the beneficial effect of estrogen therapy on muscle mass and function. Because of this, it is believed that postmenopausal women are more vulnerable to sarcopenia. Although alcohol is known to inhibit skeletal muscle protein synthesis, few studies have examined the relationship between sarcopenia and alcohol-drinking patterns.
…Study results published in the article “Associations between high-risk alcohol consumption and sarcopenia among postmenopausal women” show that the prevalence of sarcopenia was found to be nearly four times greater for the high-risk, alcohol-drinking group than the low-risk group.
…With this study suggesting that more muscle loss leads to sarcopenia and other studies suggesting that even one drink of alcohol may increase the risk of breast cancer, postmenopausal women should limit their alcohol intake.”
The therapeutic benefits of omega-3 fatty acids – which are abundant in certain fish oils – have long been known. In the 1950s, upon the discovery that omega-3 improves brain development, cod liver oil was given for free to young children, pregnant women, and nursing mothers. In the 80s, scientists reported that eskimos enjoy better coronary health than their mainland counterparts as a result of their fish rich diets. And in 2009, a study published in the Menopause journal suggested that omega-3 helps reduce the frequency of hot flushes in menopausal women.
As you can see, the hype that surround omega-3 is warranted, and not something to be shied away from.
The Truth About Fats
Many women are concerned about fat, and wrongly believe that consuming fat will make them overweight. The truth is, however, that an extremely low-fat diet won’t regulate your weight – and it certainly won’t enhance your health. Fat can be hugely beneficial in the right form, and by consuming fatty acids such as omega-3, you will surely be more healthy.
Research has confirmed that omega-3 fatty acids may have an excellent effect on impacting degenerative diseases, such as heart disease, rheumatoid arthritis, hypertension, Alzheimer’s disease, diabetes, and many more. As for menopause, omega-3 fatty acids contain anti-inflammatory properties shown to have a positive effect on many of the symptoms associated with “the change”.
What can omega-3 help with?
Because of its wonderful properties, omega-3 can greatly help women during menopause. It helps treat a range of menopausal symptoms, such as:
Hypertriglyceridemia– Postmenopausal women may have higher triglyceride concentrations than premenopausal women, exposing them to increased risk of coronary heart disease. As omega-3 offers a triglyceride-lowering effect, many practitioners recommend menopausal women obtain a bare minimum 1g/day as provided by your diet or supplementation.
Joint pain/menopause arthritis– Omega-3 fats can reduce inflammation, which may help relieve joint pain and stiffness related to menopause arthritis. Omega-3s work in a similar way as non-steroidal anti-inflammatory drugs (NSAIDs).
Menstrual pain – As part of your ovaries’ frustrating grand finale, perimenopausal women often experience strong menstrual pain and cramping. This pain is often caused by substances called prostaglandins, which come in both “good” and “bad” form. Menopause promotes the bad kind, while omega-3 fatty acids promote the good kind.
Depression– Women are twice as likely to suffer depression compared with men, and the risk is even greater following menopause. Irritability and sadness are common emotional symptoms of menopause, but omega-3 may effectively alleviate these symptoms. Omega-3s work to improve mood and restore structural integrity to brain cells that are critical in performing cognitive functions.
Osteoporosis– An increased intake of omega-3 acids increases bone mineral content and produces healthier, stronger bones. As menopause can increase a woman’s risk of developing osteoporosis due to a drop in oestrogen levels, omega-3 fatty acids should be an essential part of a menopausal diet.
Hot flushes– The frequency of hot flushes in women going through menopause can vary from as little as once a week to every 30 minutes. Some hot flushes last minutes, while others a mere few seconds. Studies have shown that while omega-3 may not affect the intensity of hot flushes, it can halve the frequency of hot flushes with the right dosage.
Vaginal dryness– Fatty acids help to lubricate the body in general, therefore helping with dryness of the vagina – a common symptom of menopause.
Brain imaging and gene analyses in twins reveal that white matter integrity is linked to an iron homeostasis gene.
Iron deficiency is a well-known cause of impaired cognitive, language, and motor development, but a report out today (January 9) in Proceedings of the National Academy of Sciences reveals that even in apparently healthy young adults, variations in iron levels correlate with variations in brain structure integrity.
“[The researchers] make a very interesting connection between the issue of iron metabolism and the integrity of white matter, more specifically myelin”—the cellular sheath that enwraps and insulates neuronal axons—said George Bartzokis of the University of California, Los Angeles, who was not involved in the study. “This would have been predicted by what is known about myelin, because it actually contains a lot of iron, so it is important that [they have] directly demonstrated this in humans with imaging.
More forgetful? Not thinking as clearly? Simple arithmetic coming more slowly? Worried that mental functions are worsening? Are the processes of ageing catching up? There is much that can be done to prevent worsening mental functioning and memory loss. For some, memory loss heralds the onset of dementia. Regardless of a person’s occupation or social environment, loss of memory is the most feared consequence of ageing…
…Specific nutritional interventions and nutritional supplements can help to detox and protect individual cells of the brain and nervous system.
Get notified about new editions
Subscribe to the Sunday Supplement
Connecting women, science and spirit, the Gynelogic Sunday Supplement delivers a bi-monthly dose of news, views and reviews, as seen through my lady lens.