Adding a ketogenic dietary intervention to IVF treatment in patients with polycystic ovary syndrome improves implantation and pregnancy
Patients with polycystic ovary syndrome (PCOS) on a high-carbohydrate diet intrinsically suffer from exacerbated glucotoxicity, insulin resistance (IR), and infertility. Lowering the carbohydrate content has improved fertility in patients with IR and PCOS; however, the effects of a well-controlled ketogenic diet on IR and fertility in PCOS patients undergoing in vitro fertilization (IVF) have not been reported.
Twelve PCOS patients with a previous failed IVF cycle and positive for IR were retrospectively evaluated. Patients followed a ketogenic diet (50 g of total carbohydrates/1800 calories/day). Ketosis was considered when urinary concentrations were > 40 mg/dL. Once ketosis was achieved, and IR diminished, patients underwent another IVF cycle. The nutritional intervention lasted for 14 ± 11 weeks. Carbohydrate consumption decreased from 208 ± 50.5 g/day to 41.71 ± 10.1 g/day, which resulted in significant weight loss (−7.9 ± 1.1 kg). Urine ketones appeared in most patients within 13.4 ± 8.1 days. In addition, there was a decrease in fasting glucose (−11.4 ± 3.5 mg/dl), triglycerides(−43.8 ± 11.6 mg/dl), fasting insulin (−11.6 ± 3.7 mIU/mL), and HOMA-IR (−3.28 ± 1.27).
All patients underwent ovarian stimulation, and compared to the previous cycle, there was no difference in oocyte number, fertilization rate, and viable embryos produced.
However, there was a significant improvement in the implantation (83.3 vs. 8.3 %), clinical pregnancy (66.7 vs. 0 %), and ongoing pregnancy/live birth rates (66.7 vs. 0 %).
Here, restriction in carbohydrate consumption in PCOS patients induced ketosis, improved key metabolic parameters, and decreased IR. Even though this did not affect oocyte or embryo quality or quantity, the subsequent IVF cycle significantly improved embryo implantation and pregnancy rates.
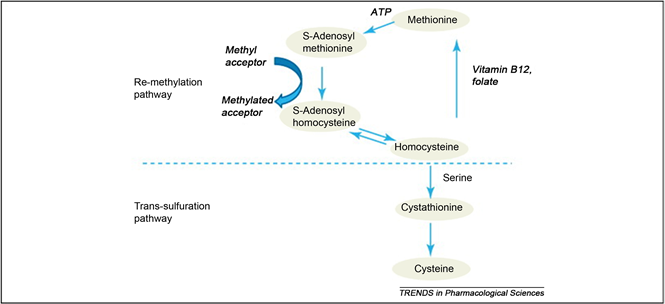
Homocysteine is an intermediate substance formed during the breakdown of the amino acid methionine and may undergo remethylation to methionine or trans-sulfuration to cystathionine or cysteine. The metabolism occurs via two pathways: remethylation to methionine, which requires folate and vitamin B12; and transsulfuration to cystathionine, which requires pyridoxal-5’-phosphate.
The disturbances in the metabolic pathways lead to the accumulation of Hcy, either by insufficient transsulfuration (through CBS mutations or vitamin B6 deficiency) or by a blockage of remethylation. In the latter case, folate or vitamin B12 deficiency may be involved, as well as MTHFR.
High levels of Hcy induce sustained injury of arterial endothelial cells, proliferation of arterial smooth muscle cells and enhance activity of key participants in vascular inflammation, atherogenesis, and vulnerability of the established atherosclerotic plaque.
Hyperhomocysteinemia has become the topic of interest in recent years. It has been highly associated with increased risk for cardiovascular disorders, such as, atherosclerosis, thromboembolism and dyslipidemia.
Women with PCOS show constellation of metabolic syndromes. Obesity, hyperandrogenemia and type 2 diabetes mellitus is the hallmark of PCOS which later becomes the risk factors for cardiovascular disease. Various studies had revealed the presence of increased Hcy level in PCOS women which may or may not be associated with other biochemical parameters. Intense treatment for PCOS can influence homocysteine levels.
Introduction
Polycystic ovary syndrome (PCOS) proves as the most common endocrine disorder with a prevalence of 5% to 15% worldwide [1] , for the women of active reproductive age, but the prevalent rate varies depending on the criteria used for the diagnosis [2] [3] . According to the Rotterdam diagnostic criteria, the prevalence rate of PCOS accounts up to 18% of reproductive-aged women [2] [3] , whilst the prevalence rate is 10% when using NIH criteria for diagnosis criteria [3] but the prevalence is still unknown in children [2] [4] . Three different criteria have been implemented for the diagnosis of PCOS: the NIH criteria (1990), the Rotterdam criteria (2003) and the Androgen and PCOS society (AE-PCOS) criteria (2006) [5] [6] . Amongst the three criteria, the Rotterdam criterion was adopted as the Practice Guidelines of the Endocrine Society [2] [7] . The Rotterdam criteria comprise features as, chronic menstrual dysfunction, clinical or biochemical hyperandrogenism and polycystic ovaries confirmed by ultrasonography (≥10 follicles and ≥10 ml ovarian volume) [8] . The etiology of PCOS still remains unclear but various predisposing genes interfere with environmental and lifestyle manners [5] [9] , makes PCOS a complex genetic disorder. The constellations of symptoms significantly affect the quality of life of PCOS women and the syndrome is associated with an increased long term risk factors such as cardiovascular disease, diabetes mellitus, infertility, cancer and psychological disorders [10] .
In current years, homocysteine, a biosynthesis of methionine has proved as a major cardinal feature of PCOS. It is a non-protein a-amino acid and cysteine homologue. Its metabolic pathway encompasses either remethylation to methionine or through transsulfuration to cystathionine as shown in Figure 1 [11] . The first metabolism pathway requires folate and vitamin B12 whereas the latter requires pyridoxal-5’-phosphate. S-adenosylmethionine (SAM) augments the synthesis of both pathways which is a moderator of methylenetetrahydrofolate reductase (MTHFR) and inhibitor of cystathionine β-synthase (CBS). The metabolic pathways are interrupted by any impaired function either by insufficient transsulfuration through CBS mutation or deficiency of vitamin B6 or secondly by remethylation blockage, can lead to abnormal accumulation of plasma Hcy. In the latter case, the accumulation of homocysteine could be due to deficiency of folate or vitamin B12, as well as MTHFR [12] .
A condition that emerges from disrupted homocysteine metabolism is hyperhomocysteinemia which has been known as the most significant risk factor for cardiovascular disease and has been confirmed by recently conducted meta-analysis study by Homocysteine Studies Collaboration [13] . Deficiencies in cystathionine beta synthase, methylenetetrahydrofolate reductase or enzymes involving methyl-B12 synthesis, as a result of a rare genetic defect, lead to severe hyperhomocysteinemia. In fasting status, due to mild impairment in the methylation mechanism (i.e. folate or B12 deficiencies or MTHFR thermolability), occurs mild hyperhomocysteinemia [12] . Homocysteine play a role as a mediator for endothelial damage and dysfunction [14] that subsequently impairs endothelial vasoreactivity and decrease endothelium thromboresistance. Hence, hyperhomocysteinemia associated with increased risk of atherosclerosis, thromoboembolic diseases and hyperinsulinemia is verified which is directly proportionate to increased risk of cardiovascular disorders with a strong correlation to insulin resistance. Hyperhomocysteinemia also aggravates the incidence of late pregnancy complications, such as preeclampsia, abruption placentae, preterm birth and intrauterine fetal death [15] . Hyperhomocysteinemia is also one of the major factors that leads to early miscarriages by impairing by interfering endometrial blood flow and vascular integrity [16] and also described as the sole variable resulting in recurrent pregnancy loss [17] .
According to numerous clinical studies, PCOS in women is associated with existence of endothelial and platelet dysfunction, minimal chronic inflammation, increased coronary artery calcification and carotid intima-media thickness in PCOS women [18] . PCOS women are highly susceptible to both cardiovascular risk factors, such as, obesity dyslipidemia, hypertension and type-2 diabetes mellitus, and mood disorders, such as depression and anxiety [2] .
Influence on Hcy Level Post PCOS Therapy
Insulin and Hcy have the ability to induce each other by inhibiting hepatic CBS [23] that results in hyperhomocysteinemia leading to compensatory hyperinsulinemia by inducing insulin resistance. This may impair activity of the MTHFR or CBS enzymes, leading to abnormal deposition of homocysteine in plasma [24] [51] [52] . This explains that insulin resistance may be the most important marker of metabolic disease in PCOS women [53] . Hence, metformin has always been the mainstay treatment for PCOS women with insulin resistance. With administration of metformin, some study has shown beneficial decrease in plasma Hcy level [8] [54] . Nonetheless, it is also studied that metformin monotherapy is unsatisfactory [55] . The study conducted by Vrbrikova et al. revealed that the treatment with metformin only may increase the plasma Hcy level [56] . Administration with rosiglitazone and metformin seem to decrease elevated oxidative stress compared to metformin treatment but no significant changes were observed in plasma Hcy [40] . Kilicdag et al. also reported the same result [57] . This statement can be explained by folate depletion and malabsorption of vitamin B12 [58] [59] that disturbs Hcy metabolism, thus, supplementation with folate can be preventative [57] [60] . Moreover, treatment with metformin and cyclic medroxyprogesterone acetate (MPA) also tend to increase Hcy level [55] . Stefano Palombo et al. reported that treatment with metformin can slightly reduce the Hcy level in PCOS women, but supplementation with folate has shown to increase the beneficial effect [60] . Hence, folate supplementation is the first therapeutic measure advised in obese PCOS patients that prevents rise in Hcy level during weight loss. A prospective randomized clinical study in 2010, in both obese and non-obese PCOS women, observed dramatic decrease in plasma Hcy level when treated with metformin. However, the study in the both group when treated with oral contraceptives increased the plasma Hcy level and other biochemical parameters that increased the metabolic risk [61] .
Statins have also been administered and seems to deplete serum Hcy levels in PCOS [48] [62] . In a prospective cohort study, the combination of ethinyl estradiol/drospirenone (EE-DRSP) and spironolactone treatment were given to lean and glucose tolerant patients with PCOS for 6 months, improved androgen excess but the combination increased Hcy level and CRP level [63] . Similarly, oral contraceptives containing 0.03 mg ethinyl estradiol and 0.15 mg desogestrel for 6 months had significantly decreased Hcy level in non-obese normoandrogenic PCOS patients [61] . Furthermore, oral contraceptives containing 35 µg ethinyl estradiol and 2 mg cyproterone acetate had resulted in rapid decrease in Hcy level in non-smoking PCOS women [64] [65] [66] , whereas Hcy level remains high in the smokers. It has also been studied that Hcy levels decreased after regular exercises for 6 months [67] and also have shown to decrease 3 months after ovarian surgery [68] .
Transmission of PCOS traits in mice occurs via an altered DNA methylation landscape
Metabolic- and inflammatory-related pathways are dysregulated in models of PCOS
Common hypomethylation signatures occur in a mouse model of PCOS and in humans
Identification of a novel epigenetic-based therapeutic strategy for PCOS
Summary
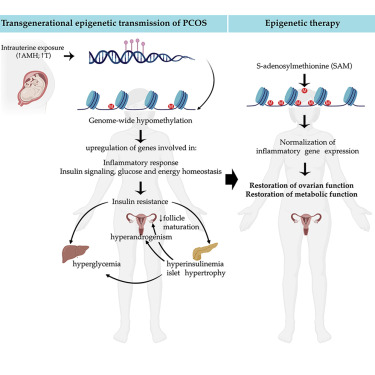
Polycystic ovary syndrome (PCOS) is the most common reproductive and metabolic disorder affecting women of reproductive age. PCOS has a strong heritable component, but its pathogenesis has been unclear. Here, we performed RNA sequencing and genome-wide DNA methylation profiling of ovarian tissue from control and third-generation PCOS-like mice.
We found that DNA hypomethylation regulates key genes associated with PCOS and that several of the differentially methylated genes are also altered in blood samples from women with PCOS compared with healthy controls. Based on this insight, we treated the PCOS mouse model with the methyl group donor S-adenosylmethionine and found that it corrected their transcriptomic, neuroendocrine, and metabolic defects.
These findings show that the transmission of PCOS traits to future generations occurs via an altered landscape of DNA methylation and propose methylome markers as a possible diagnostic landmark for the condition, while also identifying potential candidates for epigenetic-based therapy.
Discussion
We speculate that a global loss of DNA methylation, particularly in promoter-TSS and upstream-promoters, could be responsible for genomic instability in the disease condition. Consistently, a genome-wide DNA methylation study on umbilical cord blood reports a prevalence of hypomethylation in women with PCOS compared with unaffected women (Lambertini et al., 2017). As genomic instability is highly correlated with DNA damage, excessive DNA demethylation could be thus associated with impaired DNA damage repair. This is in line with many reports describing a strong association between PCOS and malignancies, such as ovarian and endometrial cancer (Escobar-Morreale, 2018), and suggest that a higher predisposition to cancer detected in women with PCOS could be due to altered DNA methylation landscapes.
Remarkably, we report that several of the differentially methylated genes identified in ovarian tissues of PCOS mice of the third generation are also altered in blood samples from women with PCOS and from daughters of women with PCOS compared with healthy women. Six genes associated with DNA demethylation (TET1), axon guidance (ROBO-1), inhibition of cell proliferation (CDKN1A), inflammation (HDC), and insulin signaling (IGFBPL1, IRS4) are hypomethylated in women with PCOS as compared with controls, and three genes (ROBO-1, HDC, and IGFBPL1) are also hypomethylated in daughters diagnosed with PCOS.
Here, we examined the therapeutic potential of SAM, a known natural agent causing methylation of several genes (Chik et al., 2014). To our knowledge, this is the first direct evidence for the potential therapeutic effect of SAM in a preclinical model of PCOS. Our investigation showed that SAM treatment can rescue the major PCOS reproductive neuroendocrine and metabolic alterations of PAMH F3 mice, thus highlighting the therapeutic potential of methylating agents as promising epigenetic therapies aimed at treating women with PCOS. We provide evidence that the methylating agent restores the aberrant expression of most inflammatory genes investigated in the ovaries as well as in metabolic tissues of PAMH F3 adult mice. Numerous studies show a causal link between low-grade inflammation and metabolic diseases, including T2D (Reilly and Saltiel, 2017). Moreover, the degree of inflammation correlates well with the severity of insulin resistance, T2D, and hyperandrogenism related to PCOS (González et al., 2006; Zhao et al., 2015).
Based on our findings we can speculate that the trigger for tissue inflammations could emanate from altered DNA methylation landscapes, which can be corrected by the SAM.
Taken together, this study points to AMH excess during gestation as a detrimental factor leading to the transgenerational transmission of PCOS cardinal neuroendocrine, reproductive, and metabolic alterations and shed lights into the epigenetic modifications underlying the susceptibility of the disease while pointing to novel diagnostic tools and epigenetic-based therapeutic avenues to treat the disease.
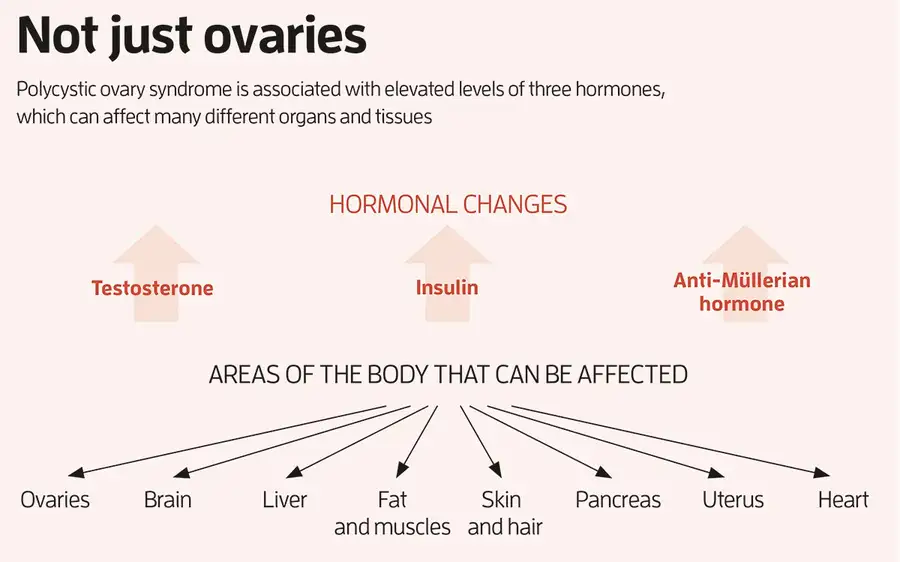
Today, a PCOS diagnosis is based on having two of three characteristic features. The first is high levels of male sex hormones like testosterone, which can cause acne, excess hair on the face and body and thinning head hair. The second is irregular or no periods, which occur because eggs often haven’t developed properly in the ovaries. This prevents their regular monthly release in the form of ovulation, meaning that it can take longer to become pregnant. The third is the presence of 20 or more “cysts” on either ovary, which are now understood to be eggs that are stuck in an immature state, rather than actual cysts.
In addition to these key features, around 50 to 70 per cent of individuals with PCOS develop resistance to insulin, which can lead to higher levels of this hormone, type 2 diabetes, weight gain, high blood pressure and heart disease. PCOS also increases the risk of endometrial and pancreatic cancer, and can cause anxiety, depression and reduced sex drive in some people.
The psychological effects may be directly caused by hormonal imbalances. Alternatively, they might arise because “if you’re a teenager, when PCOS symptoms emerge, and you’re gaining weight rapidly, you have significant acne, your periods are all over the place and you have body hair where you don’t want it, it can have a really significant impact on your self-esteem”, says Helena Teede at Monash University in Melbourne, Australia.
Finally, people with PCOS who become pregnant are more likely to have miscarriages or complications like gestational diabetes or preterm birth.
PCOS affects around 5 to 18 per cent of cis women and up to 58 per cent of trans men, although the reason why this latter figure is higher has yet to be pinned down. Despite being relatively common, it has long been one of the most neglected health conditions, says Teede. “It’s twice as common as diabetes but gets less than a hundredth of the funding,” she says. Elisabet Stener-Victorin at the Karolinska Institute in Sweden tells a similar story. “Up until about 10 years ago, I would never put ‘PCOS’ in the title of my research grant applications because it really dragged down my chances of getting funding,” she says.
Part of the problem is that it is “everybody’s business and nobody’s business”, says Teede. The many symptoms of PCOS, which vary widely between individuals, means it is managed by a range of health professionals: endocrinologists, gynaecologists, reproductive specialists, dermatologists, primary care doctors, dieticians and so on. For a long time, no one was sure who should be steering the ship and each speciality treated PCOS differently, which “constantly created confusing messages”, says Teede.
To rectify this, Teede led the development of the first international, evidence-based guidelines for PCOS, which were published in 2018. They were based on consultations with more than 3000 health professionals and people with the condition from 71 countries.
The guidelines explain how to diagnose PCOS and manage it using existing treatments. Diet and exercise interventions are recommended to begin with, since these have been shown to simultaneously improve the metabolic, reproductive and psychological features of the condition. This is because diet and exercise can assist weight loss and improve blood sugar control, which, in turn, reduce insulin and testosterone levels.
Growing evidence suggests PCOS-related hormonal imbalances during pregnancy can also have an effect on the fetus. “In a woman with PCOS, you have both the genetic factors and the in utero environment,” says Stener-Victorin. “I think it’s likely that you may carry some susceptibility genes and then you have an in utero environment that triggers its onset.” Two hormones suspected to be involved in this in utero effect are testosterone and anti-Müllerian hormone (AMH), both of which tend to be elevated in those with PCOS.
Stener-Victorin and her colleagues have found that injecting excess amounts of a form of testosterone into pregnant female mice caused their female offspring to develop many of the hallmarks of human PCOS, including irregular cycles, and greater fat mass and body weight. Similarly, when Giacobini’s team injected excess AMH into pregnant female mice, their female offspring had irregular cycles, the appearance of “polycystic” ovaries, elevated testosterone, insulin resistance, higher body weight and greater fat mass. “We now have an animal model that not only recapitulates the reproductive aspects of PCOS, but also the metabolic component seen in many women,” says Giacobini. “So, we can use these animals to really investigate the disease and design new treatment options.”
Most recently, his team discovered that the daughter mice with PCOS-like symptoms, whose mothers were injected with excess AMH during pregnancy, had altered expression of several genes involved in inflammation. This has led Giacobini to believe that PCOS is actually an inflammatory condition. His team found increased expression of inflammatory genes in the brain, ovaries, liver and fat of the mice, which he says may explain why these organs are all affected by the condition (see “Not just ovaries”, pictured above). This fits with emerging evidence of a link between inflammation and PCOS in people. A 2021 analysis led by Saad Amer at the University of Nottingham, UK, for instance, found that women with PCOS had significantly higher levels of an inflammatory marker called C-reactive protein compared with those without the condition.
Could these findings lead to new treatments? Giacobini’s team has spent the past few years developing drugs to lower AMH levels. The researchers are about to test these in mice, before hopefully progressing to human trials. “But we need to be very cautious because there are AMH receptors in different parts of the brain and a range of organs,” he says. “We cannot predict yet whether such treatment may trigger undesirable side effects until we fully comprehend the role of AMH in all those organs.” Interestingly, AMH declines with age, which may explain why some with PCOS who were unable to conceive naturally in their 20s and 30s are able to do so in their 40s, when their AMH levels fall into the normal fertility range, says Giacobini. This delayed fertility window could also be the reason why those with PCOS reach menopause four years later than average.
Another treatment option may be drugs that correct the altered expression of inflammatory and other genes implicated in PCOS, says Giacobini. Last year, his team showed thatPCOS-like symptoms could be reversed in female mice by giving them a drug called S-adenosylmethionine that corrected the altered gene expressions. This drug couldn’t be safely given to people because it affects too many other genes, but it may be possible to develop more tailored treatments in the future, says Giacobini.
Teede says these approaches are worth pursuing, but cautions against extrapolating too far from animal studies. “PCOS is not caused by one mechanism, it’s multiple mechanisms that add up together,” she says. “If you’ve got an animal model that uses one mechanism to induce a PCOS-like status, you might be able to reverse that one mechanism, but treating a complex multifactorial condition in humans is harder.”
Misleading moniker
Is it time to rename polycystic ovary syndrome? There is a growing push to do so since it is now recognised as a whole-body condition, people can be diagnosed with it even if they don’t have “polycystic” ovaries and we now know that the “cysts” are undeveloped eggs, not actual cysts.
“We desperately need a name change,” says Helena Teede at Monash University in Melbourne, Australia. “The name should reflect what it actually is. Having a name around the ovaries misses the diversity of the condition.”
Teede and her colleagues are consulting health professionals and people with the condition to agree on a new name – the most preferred one at this stage is “reproductive metabolic syndrome”.
They hope to formalise this name change in the middle of this year when they release an updated version of the international guidelines on the diagnosis and treatment of the condition.
Objective: To identify clinical, laboratory and molecular genetic predictors of menstrual circle regulation in patients with polycystic ovary syndrome (PCOS) undergoing metformin treatment.
Materials and methods: The study included 143 women with PCOS (mean age is 26.4±4.6 years, mean body mass index is 23.8 (4.8) kg/m2). The assessment of androgen profile and levels of AMH, LH, FSH was performed before and 6 months after the treatment. Also, 2-hour oral glucose tolerance test with insulin level examination and dual-energy X-ray absorptiometry were done. Single-nucleotide polymorphisms (SNPs) were genotyped using polymerase chain reaction and next generation sequencing for 45 loci. All patients were administered metformin (Glucophage Long) 1500 mg/day with dose titration for 6 months. Depending on the response to the therapy, the patients were divided into two groups:
group 1 included 70 (53.1%) patients whose menstrual cycle was regulated,
group 2 consisted of 48 (36.3%) patients without any effect of therapy;
14 (10.6%) patients with partial response to therapy were not included in the analysis of predicting the effectiveness of the treatment.
Results: The following independent predictors of the effectiveness of metformin therapy in PCOS were revealed:
AMH level less than 13.3 ng/ml,
total testosterone level less than 1.81 ng/ml,
index of adipose tissue distribution A/G less than 0.90, as well as
polymorphism of loci in the genes SLCO1B1 (rs4149056), ACE (rs4340), FSHR (rs2349415), OST1 (rs113569197).
The model which was developed for predicting menstrual cycle regulation in patients with PCOS undergoing metformin therapy included the baseline level of AMH and rs2349415 SNPs of FSHR gene.
Conclusion: The most significant factors determining metformin effectiveness in PCOS patients were AMH level and genotype С/С of FSHR (rs2349415).
Objective. To reveal taurine`s effects on metabolism, menstrual and reproductive function in women with PCOS.
Methods. A total of 44 women with PCOS were included in the study with ages ranging from 18 to 44. Patients were randomized into two groups:
1) Dibicor group, n=30;
2) Placebo group, n=14.
Thirty patients received dibicor 500 mg twice a day, fourteen patients received placebo 500 mg twice a day. Duration of the therapy was 3 months. Anthropometric measurements, content of adipose tissue, blood pressure, pulse rate, lipid levels, 3-hours oral glucose tolerance test (OGTT, 75 gr glucose), ultrasound uterine and ovarian investigations were done both before and after the therapy.
Results. In the study group systolic and diastolic blood pressures were decreased. Heart rate was decreased, while serum HDL cholesterol was significantly increased (p=0,03). Changes in glucose metabolism characterized with metabolic clearance improvement in peripheral tissue due to increasing of insulin sensitivity and beta cell function. Modulation of metabolism with taurine was accompanied by ovarian function enhancement, normalization of menstrual cycle, formation of dominate follicle in 20% of women with previous history of anovulation.
Conclusion. Administration of dibicor in women with PCOS modulates metabolic dysfunction and improves reproductive prognosis, and also has protective effects against diabetes and cardiovascular diseases.
Polycystic ovary syndrome (PCOS) increases type 2 diabetes and non-alcoholic fatty liver disease (NAFLD) with insulin resistance. We hypothesized that a 35 g whey preload would improve insulin sensitivity and glucose handling while reducing biomarkers associated with NAFLD.
Twenty-nine age-matched women (CON = 15, PCOS = 14) completed oral glycemic tolerance tests following baseline (Day 0) as well as an acute (Day 1) and short-term whey supplementation (Day 7). Whey had an interaction effect on glucose (p = 0.02) and insulin (p = 0.03), with glucose remaining stable and insulin increasing with whey supplementation.
Insulin sensitivity (p < 0.01) improved with whey associated with increased glucagon secretion (p < 0.01). Alanine aminotransferase (ALT), and aspartate aminotransferase (AST) remained unchanged, but “day” had an effect on the AST:ALT ratio (p = 0.04), whereas triglycerides and sex hormone binding globulin overall were greater in the PCOS group (p < 0.05). Total cholesterol decreased in PCOS (by 13%) and CON (by 8%) (NS). HepG2 cells treated with plasma from participants before and after whey decreased lipid accumulation in the PCOS group after whey (p < 0.05).
Whey provided an insulinogenic and glycemic homeostatic effect in women with PCOS with the potential to combat NAFLD-consequences.
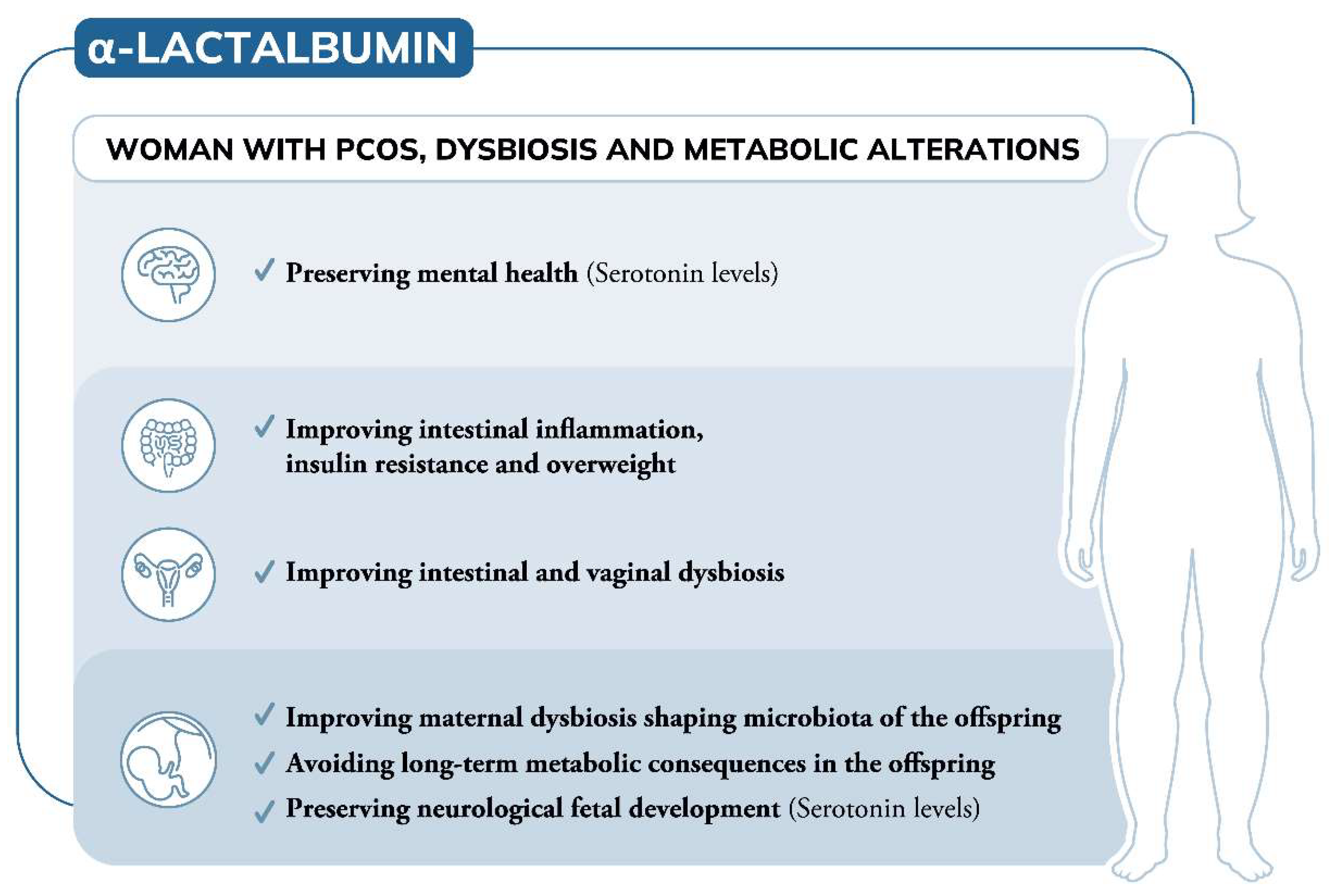
To date, the involvement of α-Lactalbumin (α-LA) in the management of polycystic ovary syndrome (PCOS) refers to its ability to improve intestinal absorption of natural molecules like inositols, overcoming the inositol resistance. However, due to its own aminoacidic building blocks, α-LA is involved in various biological processes that can open new additional applications.
A great portion of women with PCOS exhibit gastrointestinal dysbiosis, which is in turn one of the triggering mechanisms of the syndrome. Due to its prebiotic effect, α-LA can recover dysbiosis, also improving the insulin resistance, obesity and intestinal inflammation frequently associated with PCOS. Further observations suggest that altered gut microbiota negatively influence mental wellbeing.
Depressive mood and low serotonin levels are indeed common features of women with PCOS. Thanks to its content of tryptophan, which is the precursor of serotonin, and considering the strict link between gut and brain, using α-LA contributes to preserving mental well-being by maintaining high levels of serotonin.
In addition, considering women with PCOS seeking pregnancy, both altered microbiota and serotonin levels can induce later consequences in the offspring. Therefore, a deeper knowledge of potential applications of α-LA is required to transition to preclinical and clinical studies extending its therapeutic advantages in PCOS.
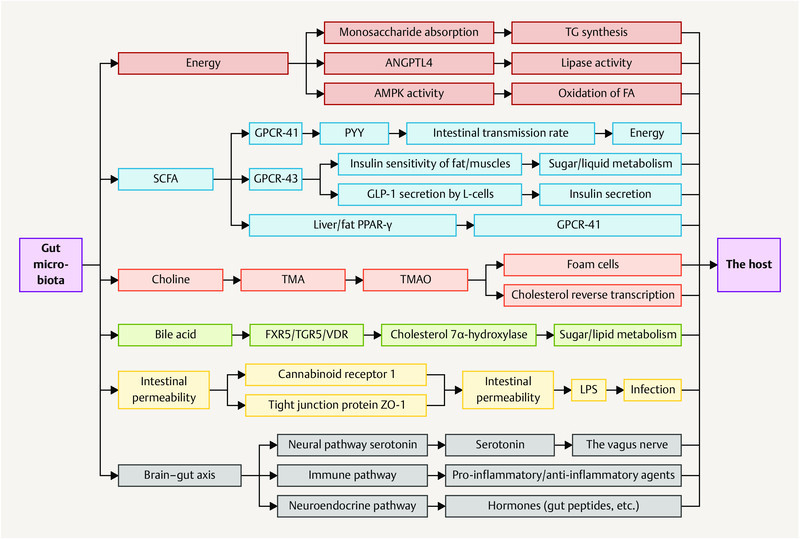
Polycystic ovary syndrome (PCOS) is an endocrine and metabolic syndrome (MS) with a complex etiology, and its pathogenesis is not yet clear. In recent years, the correlation between gut microbiota (GM) and metabolic disease has become a hot topic in research, leading to a number of new ideas about the etiology and pathological mechanisms of PCOS.
The literature shows that GM can cause insulin resistance, hyperandrogenism, chronic inflammation and metabolic syndrome (obesity, diabetes) and may contribute to the development of PCOS by influencing energy absorption, the pathways of short chain fatty acids (SCFA), lipopolysaccharides, choline and bile acids, intestinal permeability and the brain–gut axis.
As part of the treatment of PCOS, fecal microbiota transplantation, supplementation with prebiotics and traditional Chinese medicine can be used to regulate GM and treat disorders.
This article reviews possible mechanisms and treatment options for PCOS, based on methods which target the GM, and offers new ideas for the treatment of PCOS.
The key gut microbial biomarkers for polycystic ovarian syndrome (PCOS) and how dysbiosis causes insulin resistance and PCOS remain unclear.
Objective: To assess the characteristics of intestinal flora in PCOS and explore whether abnormal intestinal flora can affect insulin resistance and promote PCOS and whether chenodeoxycholic acid (CDCA) can activate intestinal farnesoid X receptor (FXR), improving glucose metabolism in PCOS.
Results: Bacteroides was significantly enriched in treatment-naïve PCOS patients. The enrichment in Bacteroides was reproduced in the PCOS mouse model. Gut microbiota removal ameliorated the PCOS phenotype and insulin resistance and increased relative FXR mRNA levels in the ileum and serum fibroblast growth factor 15 levels. PCOS stool-transplanted mice exhibited insulin resistance at 10 weeks but not PCOS. Treating the PCOS mouse model with CDCA improved glucose metabolism.
Conclusions: Bacteroides is a key microbial biomarker in PCOS and shows diagnostic value. Gut dysbiosis can cause insulin resistance. FXR activation might play a beneficial rather than detrimental role in glucose metabolism in PCOS.
Eight patients with PCOS displaying oligo-amenorrhea from at least 1 yr underwent a combined treatment with N-acetylcysteine (NAC) (1200 mg/die) plus L-arginine (ARG) (1600 mg/die) for 6 months.
Menstrual function, glucose and insulin levels, and, in turn, homeostasis model assessment (HOMA) index were monitored.
Menstrual function was at some extent restored as indicated by the number of uterine bleedings under treatment.
Also, a well-defined biphasic pattern in the basal body temperature suggested ovulatory cycles. The HOMA index decreased under treatment.
In conclusion, this preliminary, open study suggests that prolonged treatment with NAC+ARG might restore gonadal function in PCOS. This effect seems associated to an improvement in insulin sensitivity.
Infertility affects as many as 12.3% of women ages 15-44 (or 7.5 million women) in the United States.
Consequently, it is imperative to find methods to help women overcome infertility so that they may conceive a healthy child.
Many of the current treatments for infertility are costly, have low success rates, and have the potential to negatively affect long-term health. The common medical interventions used for infertility include fertility medications, in-vitro fertilization (IVF), and intrauterine insemination (IUI). Fertility medications, such as clomiphene and gonadotropins, stimulate growth of the ovarian follicle, followed by follicular rupture induced by a human chorionic gonadotropin (hCG) trigger shot.
These medications are often used in conjunction with IVF and IUI. IVF is an assisted reproductive technology that includes combining an egg and a sperm in a laboratory and then transferring the fertilized embryo into the uterus. IUI involves placing the sperm inside of the uterus to help with fertilization. Although less invasive and expensive than IVF, in IUI the sperm has to fertilize the egg on its own within the woman’s reproductive tract.
Research suggests a link between a variety of health conditions and subsequent infertility, including polycystic ovarian syndrome (PCOS), endometriosis, advanced maternal age (AMA), high body mass index (BMI), the MTHFR genetic mutation, hypothyroidism (both clinical and subclinical), and poor ovarian reserve.
In this article, we provide case evidence for alternative methods for managing infertility that are effective at improving the underlying condition leading to infertility – methods that are less expensive than medical intervention and are supportive of long-term health.
Polycystic ovary syndrome (PCOS) is a complex and common endocrine disorder characterized by hyperandrogenism, which is accompanied by follicle growth arrest at the small antral stage, minimal granulosa cell proliferation, and chronic anovulation.
Polyunsaturated fatty acids (PUFAs) are necessary for the body’s metabolism, growth and development. Although PUFAs play an important role in the regulation of female reproduction, their role in ovarian development in PCOS is still unclear.
The present study was conducted to investigate the effects of different ratios of n-3/n-6 PUFAs (omega-3/omega-6) on ovary development in PCOS rats. Serum levels of reproductive hormones and enzymes related to steroidogenesis were assessed.
The results indicated that PUFAs (n-3/n-6: 1/15) significantly increased ovarian weight and improved the ovarian structure although they had no significant effect on body weight in PCOS rats.
Meanwhile, apoptosis was attenuated accompanied by increased cell proliferation by PUFAs (n-3/n-6: 1/15). Moreover, serum levels of hormones (FSH and E2) were also significantly increased by PUFAs (n-3/n-6: 1/15) accompanied by decreased T levels.
To investigate whether PUFAs regulate the expression of enzymes related to hormone synthesis, western blotting was used to determine the protein levels of CYP51, CYP19, StAR and 3β-HSD.
The results showed that PUFAs significantly increased the protein levels of all of these enzymes. These results indicate that PUFAs enhance the reproductive performance of PCOS by increasing the expression of steroidogenesis enzymes, which are related to hormone secretion and ovarian functions.
These findings provide evidence that a balanced n-3/n-6 PUFA ratio is beneficial for PCOS reproduction.
Polycystic ovarian syndrome (PCOS) is a common endocrine disease across the world. Because gut microbiota play a key role in the pathogenesis of PCOS, probiotics may alleviate PCOS symptoms through the regulation of intestinal flora. The effects of 8 lactic acid bacterial strains on PCOS were investigated. Letrozole was used to produce a PCOS rat model and a 4-week-strain-intervention was performed. Diane-35, as a clinical PCOS treatment medicine, was effective in attenuating rats’ reproductive disorders.
Lactobacillus plantarum HL2 was protective against ovary pathological changes and restored luteinizing hormone, follicle stimulating hormone and testosterone levels.
Bifidobacterium longum HB3 also alleviated ovary abnormalities and decreased testosterone levels.
Administration of lactic acid bacteria up-regulated short-chain fatty acid levels.
Based on 16S rRNA sequencing, lactic acid bacteria improved letrozole induced gut microbiota dysbiosis with different degrees.
Akkermansia, Roseburia, Prevotella, Staphylococcus and Lactobacillus genera were correlated with sex hormone levels. Some of the sex hormone-related gut microbiota were restored by treatment with the strains.
These results demonstrated that lactic acid bacteria alleviated PCOS in a rat model by regulating sex hormone related gut microbiota. Modifying gut microbiota by probiotic interventions may thus be a promising therapeutic option for PCOS.
Polycystic ovary syndrome (PCOS) is characterized by androgen excess, ovulatory dysfunction and polycystic ovaries1, and is often accompanied by insulin resistance2.
The mechanism of ovulatory dysfunction and insulin resistance in PCOS remains elusive, thus limiting the development of therapeutics. Improved metabolic health is associated with a relatively high microbiota gene content and increased microbial diversity3,4.
This study aimed to investigate the impact of the gut microbiota and its metabolites on the regulation of PCOS-associated ovarian dysfunction and insulin resistance. Here, we report that Bacteroides vulgatus was markedly elevated in the gut microbiota of individuals with PCOS, accompanied by reduced glycodeoxycholic acid and tauroursodeoxycholic acid levels.
Transplantation of fecal microbiota from women with PCOS or B. vulgatus-colonized recipient mice resulted in increased disruption of ovarian functions, insulin resistance, altered bile acid metabolism, reduced interleukin-22 secretion and infertility.
Mechanistically, glycodeoxycholic acid induced intestinal group 3 innate lymphoid cell IL-22 secretion through GATA binding protein 3, and IL-22 in turn improved the PCOS phenotype.
This finding is consistent with the reduced levels of IL-22 in individuals with PCOS. This study suggests that modifying the gut microbiota, altering bile acid metabolism and/or increasing IL-22 levels may be of value for the treatment of PCOS.
Fat tissue in women with polycystic ovary syndrome produces an inadequate amount of the hormone that regulates how fats and glucose are processed, promoting increased insulin resistance and inflammation, glucose intolerance, and greater risk of diabetes and heart disease, according to this study.
Fat tissue is the body’s largest hormone-producing organ, secreting a large number of hormones that affect appetite, bowel function, brain function, and fat and sugar metabolism. One of these hormones is adiponectin, which in sufficient quantities encourages the proper action of insulin on fats and sugars and reduces inflammation. Women with PCOS produce a smaller amount of adiponectin than women who do not have the disease, in response to other fat-produced hormones, according to the research to be published in the February issue of Journal of Clinical Endocrinology and Metabolism.
While Polycystic Ovary Syndrome is often associated with obesity, women with the disorder are not necessarily more likely to be overweight. In fact, in the study, adiponectin was lacking in PCOS patients whose weight was considered to be in a healthy range, as well as in those patients who were overweight.
PCOS also can cause symptoms such as irregular ovulation and menstruation, infertility, excess male hormones, excess male-like hair growth (hirsutism), and polycystic ovaries. About two-thirds of women with PCOS have insulin resistance, an impairment in the effectiveness of the hormone insulin, which regulates the body’s utilization of fats and sugars, and which results in a higher risk for diabetes, metabolic syndrome, and cardiovascular disease.
Get notified about new editions
Subscribe to the Sunday Supplement
Connecting women, science and spirit, the Gynelogic Sunday Supplement delivers a bi-monthly dose of news, views and reviews, as seen through my lady lens.