To prove the efficacy of oral vitamin B1 administration for the treatment of primary dysmenorrhoea, a randomised, double-blind, placebo-controlled study was carried out on 556 girls aged 12-21 yr, having moderate to very severe spasmodic dysmenorrhoea.
Thiamine hydrochloride (vitamin B1) was given in a dose of 100 mg orally, daily for 90 days.
The combined final results of both the ‘active treatment first’ group and the ‘placebo first’ group, after 90 days of vitamin B1 administration, were
87 per cent completely cured,
8 per cent relieved (pain almost nil to reduced)
5 per cent showed no effect whatsoever.
The results remained the same two months later as well when no drug was administered. Unlike all the current treatments which are suppression-oriented, this curative treatment directly treats the cause, is free from side effects, is inexpensive and easy to administer.
Seeing blood spots in your underwear when your period ended days ago can feel puzzling and concerning. Known as intermenstrual bleeding, spotting between periods and ovulation is not normally cause for alarm. But in some cases, it can indicate an underlying vaginal infection needs treatment.
The most common culprits of bleeding between cycles are bacterial vaginosis (BV), yeast infections, and sexually transmitted diseases like chlamydia and gonorrhea. Here’s an overview of how these infections lead to spotting:
Bacterial Vaginosis – Caused by an overgrowth of bad bacteria, BV leads to vaginal inflammation and thinning of the lining. This makes the walls more prone to bleeding. A fishy odor is a hallmark of BV.
Yeast Infections – Candida fungus irritates the vaginal tissue, causing itchiness and redness. Scratching can disrupt the sensitive lining enough to cause minor bleeding. Yeast infections produce thick, white discharge.
Chlamydia and Gonorrhea – STDs like these infect the cervix, which can become friable and bleed easily. Pain during sex is also common with chlamydia and gonorrhea.
Trichomoniasis – This STD invades the vagina, creating an environment prone to spotting and bleeding. A smelly, greenish-yellow discharge occurs with trichomoniasis.
Rising oestrogen levels approaching ovulation create an environment in the vagina that promotes the growth of bad bacteria and yeast. The hormonal changes make women more susceptible to infections during this time of the cycle.
While usually not severe, vaginal infections should always be treated properly. The first step is to test for any infections. My preferred options are at a local sexual health clinic, making sure that also include a test for BV, or I can order the Vaginal Ecologix test for you, and you can gain a comprehensive picture of your vaginal microbiome and identify specific infections.
In most cases, vaginal infection-related bleeding is short-lived once treated. But if you ever experience heavy, persistent bleeding between cycles, seek medical care promptly.
So don’t ignore sporadic spotting. It may be your body’s signalling an underlying infection needing attention. With proper treatment, you can restore healthy vaginal flora, tissue, and pH balance.
Chronic insomnia disorder is one of the most common problems in postmenopausal women, exacerbated by underdiagnosis and improper treatment.
This double-blinded, randomized, placebo-controlled trial was conducted to evaluate the potential of vitamin E to treat chronic insomnia as an alternative to sedative drugs and hormonal therapy.
The study enrolled 160 postmenopausal women with chronic insomnia disorder, divided randomly into two groups. The vitamin E group received 400 units of mixed tocopherol daily, while the placebo group received an identical oral capsule.
The primary outcome of this study was sleep quality assessed by the Pittsburgh Sleep Quality Index (PSQI), a self-evaluated and standardized questionnaire. The secondary outcome was the percentage of participants using sedative drugs. There were no significant differences in baseline characteristics between the study groups. However, the median PSQI score at baseline was slightly higher in the vitamin E group compared with the placebo. After one month of intervention, the PSQI score was significantly lower (indicating better sleep quality) in the vitamin E group compared with the placebo.
Moreover, the improvement score was significantly higher in the vitamin E group compared with the placebo. In addition, there was a significant reduction in the percentage of patients using sedative drugs in the vitamin E group (15%), while this reduction was not statistically significant in the placebo group (7.5%).
This study demonstrates vitamin E’s potential as an excellent alternative treatment for chronic insomnia disorder that improves sleep quality and reduces sedative drug use.
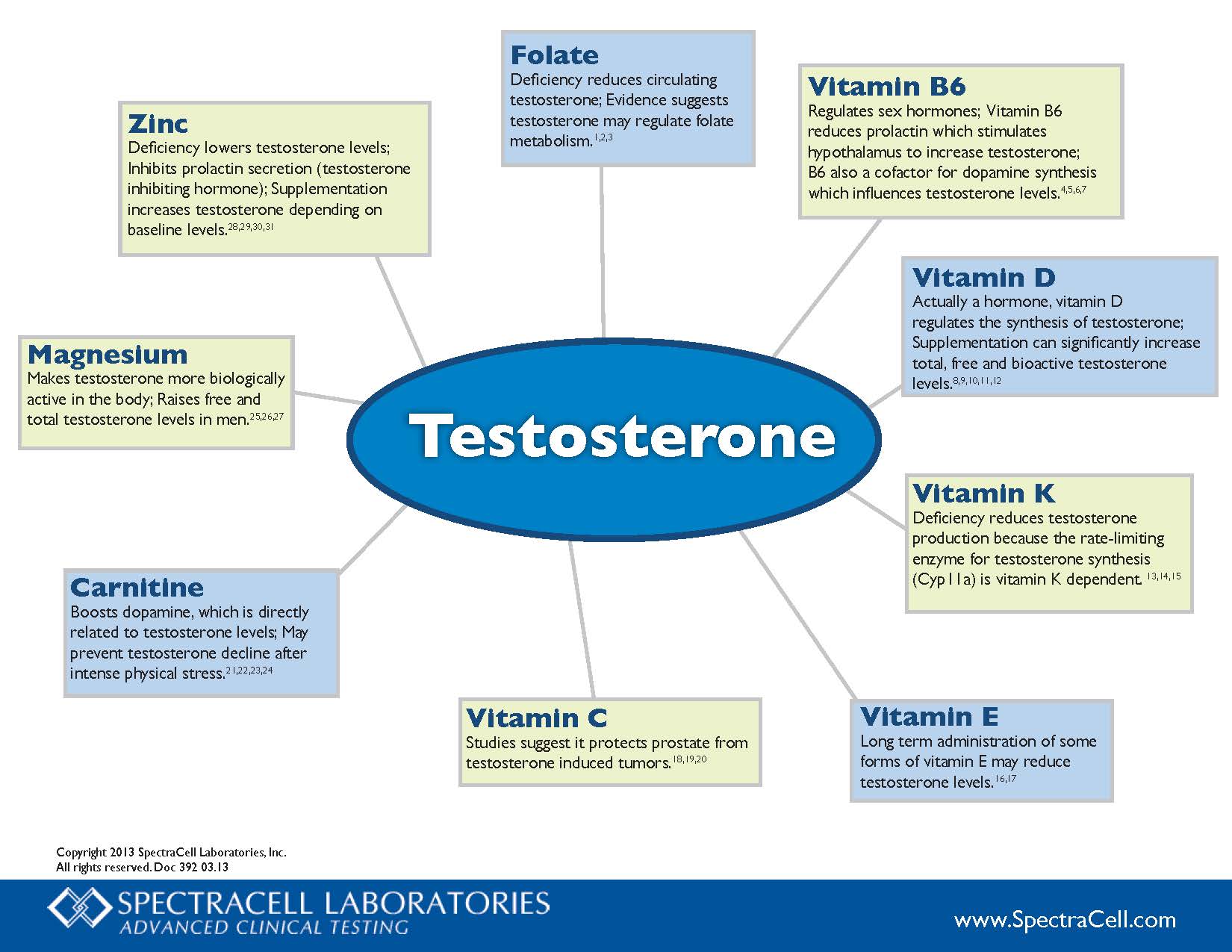
Vitamin B6 Regulates sex hormones; Vitamin B6 reduces prolactin which stimulates hypothalamus to increase testosterone; B6 also a cofactor for dopamine synthesis which influences testosterone levels.4,5,6,7
Vitamin D Actually a hormone, vitamin D regulates the synthesis of testosterone; Supplementation can significantly increase total, free and bioactive testosterone levels. 8,9,10,11,12
Vitamin K Deficiency reduces testosterone production because the rate-limiting enzyme for testosterone synthesis (Cyp11a) is vitamin K dependent. 13,14,15
Vitamin E Long term administration of some forms of vitamin E may reduce testosterone levels.16,17
Vitamin C Studies suggest it protects prostate from testosterone induced tumors.18,19,20
Carnitine Boosts dopamine, which is directly related to testosterone levels; May prevent testosterone decline after intense physical stress.21,22,23,24
Magnesium Makes testosterone more biologically active in the body; Raises free and total testosterone levels in men.25,26,27
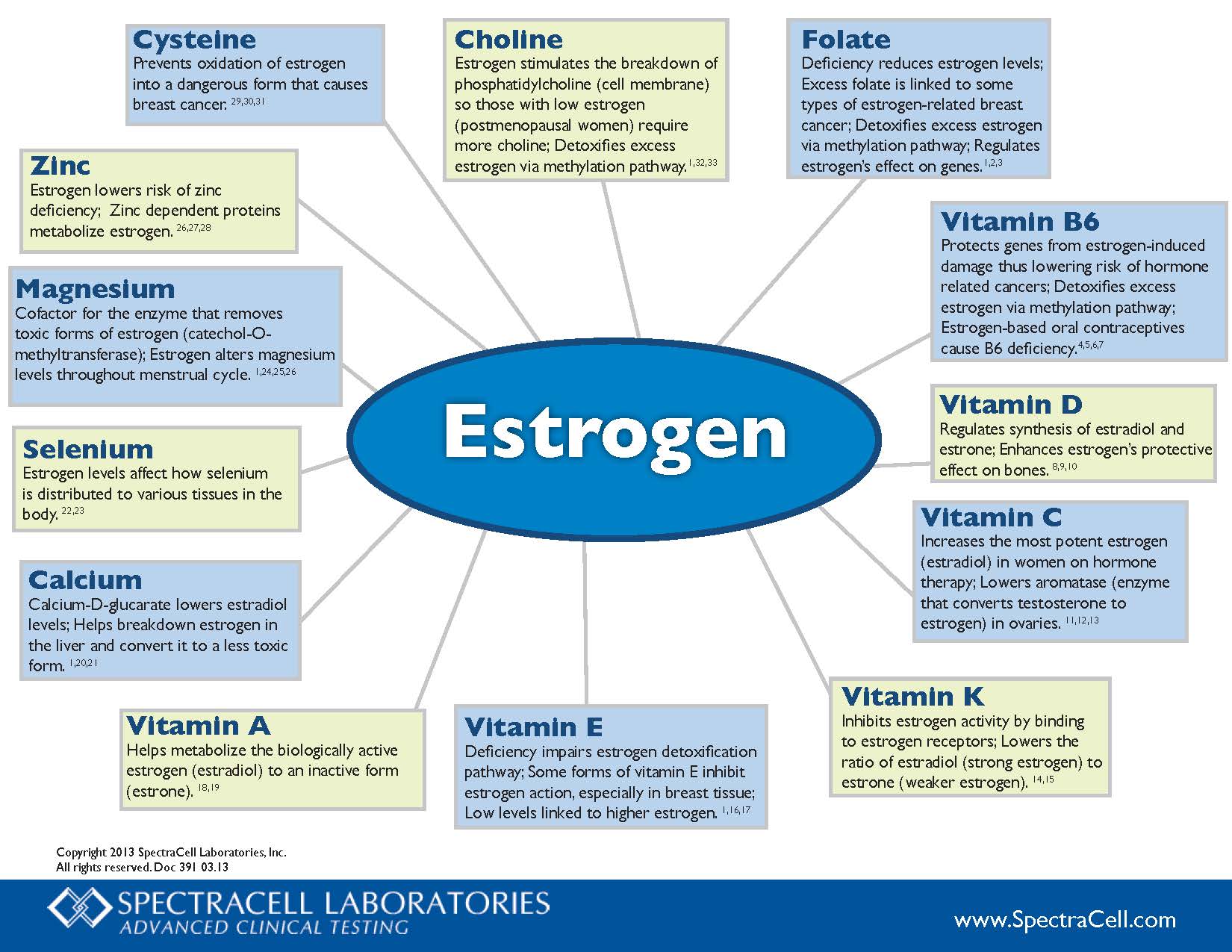
Choline – Estrogen stimulates the breakdown of phosphatidylcholine (cell membrane) so those with low estrogen (postmenopausal women) require more choline; Detoxifies excess estrogen via methylation pathway.1,32,33
Folate – Deficiency reduces estrogen levels; Excess folate is linked to some types of estrogen-related breast cancer; Detoxifies excess estrogen via methylation pathway; Regulates estrogen’s effect on genes.1,2,3
Vitamin B6 – Protects genes from estrogen-induced damage thus lowering risk of hormone related cancers; Detoxifies excess estrogen via methylation pathway; Estrogen-based oral contraceptives cause B6 deficiency.4,5,6,7
Vitamin D – Regulates synthesis of estradiol and estrone; Enhances estrogen’s protective effect on bones.8,9,10
Vitamin C – Increases the most potent estrogen (estradiol) in women on hormone therapy; Lowers aromatase (enzyme that converts testosterone to estrogen) in ovaries.11.12.13
Vitamin K – Inhibits estrogen activity by binding to estrogen receptors; Lowers the ratio of estradiol (strong estrogen) to estrone (weaker estrogen).14,15
Vitamin E – Deficiency impairs estrogen detoxification pathway; Some forms of vitamin E inhibit estrogen action, especially in breast tissue; Low levels linked to higher estrogen.1,16,17
Vitamin A – Helps metabolize the biologically active estrogen (estradiol) to an inactive form (estrone).18,19
Calcium – Calcium-D-glucarate lowers estradiol levels; Helps breakdown estrogen in the liver and convert it to a less toxic form.1,20,21
Selenium – Estrogen levels affect how selenium is distributed to various tissues in the body.22,23
Magnesium – Cofactor for the enzyme that removes toxic forms of estrogen (catechol-O-methyltransferase); Estrogen alters magnesium levels throughout menstrual cycle.1,24,25,26
For some women, reaching the menopause can be one of life’s milestones, but when it will happen is a big unknown. Now a blood test can help predict when a woman’s last menstrual period is likely to be.
The test, called MenoCheck, can’t give a firm date, but it can tell women who are over 47 if they are likely to stop having periods within the next year. It would be most useful for those considering being sterilised or having surgery for painful or heavy periods, says Nanette Santoro at the University of Colorado Medical School in Aurora. “They may be wondering how much longer they have to put up with this.”
The average age at which menopause occurs is 51, but in most cases, it can happen any time from a person’s forties to early sixties. Periods usually become more infrequent before stopping for good. They stop because the ovaries run out of functioning eggs, which leads to lower levels of anti-Mullerian hormone – a chemical made by eggs – in blood.
Previous tests haven’t been able to measure the very low levels of anti-Mullerian hormone present in the year or two before menopause. But MenoCheck, which has been on sale for about a year, is more sensitive. To see how well it does, Santoro’s team used it on blood samples taken at yearly intervals from about 1500 women taking part in a different menopause study. Santoro is a consultant for MenoCheck’s manufacturer Ansh Labs.
The team found that those over 47 whose anti-Mullerian hormone level was below a certain cut-off had a 67 per cent chance of having their last period within the next year, and an 82 per cent chance of having it within two.
Most women wouldn’t need to take the test to know that they are nearing the menopause, says Esther Eisenberg at the US’s National Institutes of Health.
Yet without it, women can only be advised that if their periods have started to become irregular, they are likely to stop completely within four years, says Santoro.
Menopause is associated with increased risks for cardiovascular disease, osteoporosis, and cancer. Many women experience declining energy, mood, cognitive function and memory during menopause.
Rhodiola rosea extracts have been shown to enhance mood, cognitive function, and memory. Moreover, these extracts possess anti-stress, neuroprotective, cardiovascular-protective, and anticarcinogenic properties, which are particularly valuable to counteract some of the common health risks seen in women as they age. R. rosea is low in side effects compared to synthetic selective estrogen receptor modulators (SERMS).
Preclinical and clinical studies suggest that R. rosea extracts provide a combination of effects that could counteract the adverse consequences of estrogen decline by improving neurological, endothelial, and cardiovascular functions.
As a natural SERM, R. rosea could alleviate menopause-related symptoms while conferring additional neuro-protective, cardio-protective, anti-stress, anti-fatigue, osteoprotective, and other health benefits.
Unlike HRT, preliminary evidence indicates that orally ingested R. rosea extracts are unlikely to cause estrogenic effects or increased the risk of cancer in hormone sensitive tissues. R. rosea extracts and salidroside do not significantly stimulate, but rather inhibit growth of human breast cancer in vitro and in vivo in some studies. Human studies are needed to verify the safety of R. rosea in postmenopausal women who are at increased risk or who are being treated for breast cancer.
Further research on the use of R. rosea alone and in combination with other adaptogens during menopause would enable development of this promising alternative SERM.
Endometriosis is a chronic gynecologic disease process with multifactorial etiology. Increased oxidative stress, a result of increased production of free radicals or depletion of the body’s endogenous antioxidant defense, has been implicated in its pathogenesis. Oxidative stress is thought to promote angiogenesis and the growth and proliferation of endometriotic implants. Oxidative stress in the reproductive [...]
Endometriosis is a chronic gynecologic disease process with multifactorial etiology. Increased oxidative stress, a result of increased production of free radicals or depletion of the body’s endogenous antioxidant defense, has been implicated in its pathogenesis. Oxidative stress is thought to promote angiogenesis and the growth and proliferation of endometriotic implants. Oxidative stress in the reproductive tract microenvironment is known to negatively affect sperm count and quality and may also arrest fertilized egg division leading to embryo death. Increased DNA damage in sperm, oocytes, and resultant embryos may account for the increase in miscarriages and fertilization and implantation failures seen in patients with endometriosis.
The evidence linking endometriosis and infertility to endogenous pro-oxidant imbalance provides a rationale for the empiric use of antioxidant therapy. Vitamin C and E deficiency has been demonstrated in women with endometriosis. Observational and randomized controlled studies have shown vitamin C and E combination therapy to decrease markers of oxidative stress.
Reversal of severe chronic acne and premenstrual symptoms including uncontrollable anger, anger and mood swings, affecting work and family relationships.
Overview
Acne is most prevalent in teenage years, and when it continues into adulthood it can cause can cause much ongoing distress. In addition to permanent scarring and disfigurement, acne has long-lasting psychosocial effects that affect quality of life.
Acne often presents in rhythm with menstrual cycles, particularly before the onset of menstruation in combination premenstrual syndrome (PMS), indicating hormonal involvement.
There are many natural approaches to consider that have been shown to be effective for helping women resolve their acne and PMS, but are not always understood by primary healthcare practitioners where topical drugs, antibiotics or the pill are the current medical treatments.
Introduction
BA was 33 years old and working as a solicitor when she came to see me saying:
She said:
“Since the age of 13 I have been suffering from what I think is cystic acne. At that age, once every 6 months or so, I would get one massive spot on my face. As the years have progressed, this has become much more frequent and appear to be more prevalent on my cheeks and jawline. Now, about 10 days before my period, massive cysts develop under my skin. Sometimes they are solid and other times they pop. It causes me severe anxiety and has had had an affect on my mood, social life and confidence.
I’ve been taking antibiotics every other month for the last 4-5 years but they’re not helping.
I also find that 7-10 days before my period I go completely bonkers – my mood, tolerance and anger levels are beyond my control. I feel out of control and unable to deal with my emotions rationally. As soon as my period starts, I have a sense of relief. This is having a negative impact on my husband and my children. I am struggling with my relationships.”
Health history
Cystic acne started a 13
She was prescribed Lymacyline (a tetracyline antibiotic), Clamidamice (an antibiotic which is given to treat serious bacterial infections), Roaccutane (a vitamin A derivative with multiple side effects), and Yazmin (a contraceptive pill). None of these were effective and her acne was getting progressively worse.
20: began a stressful career and started feeling anxiety, low patience, irritability, feeling angry, emotional and tearful. She had bouts of severe mood swings and uncontrollable anger.
Her periods were very heavy in the first 2 days and then flow was normal.
Painful periods
Ovulation was painful
She experience bloating after carbohydrates.
Nutrition history
BA’s diet was high in sugar and carbohydrates, and she frequently had sugar cravings, especially on her period.
Her nutrition was was low on protein and water
She ate dairy 2-3 times a month.
Significant test results
MARKER
LEVEL
INTERPRETATION
Vitamin D
Severe deficiency
Low immune function Oestrogen too high
Creatinine
Low
Impaired methylation and liver detoxification of oestrogen
Bilirubin
High
Impaired liver function
Ferritin
High
Inflammation
Haemoglobin
Low
Iron deficiency
HbA1c
High
Insulin resistance / pre-diabetes
Root cause analysis
Acne
Acne is mediated by high testosterone levels, stimulated by insulin resistance/spikes mediated by high sugar/starch intake, and dairy via Insulin Growth factor.
PMS
BA’s oestrogen was too high as evidenced by heavy bleeding and ovulation pain.
Excess oestrogen symptoms additionally include premenstrual anxiety, acne and mood swings.
I recommended a low carbohydrate, moderate protein, high fat nutrition plan which was rich in fish and eggs, with a high level of vegetables and beneficial fats, and personalised to BA’s requirements.
Avoidance of all cow’s dairy foods.
BA was asked to follow my 7 food rules as closely as possible.
LIFESTYLE
BA was recommended to use pumpkin seed oil as a cleanser twice a day, applying a teaspoon of the oil to her face and removing with a damp microfibre cloth. After cleansing I recommended she apply vitamin B3 serum.
SUPPLEMENTS
Vitamin D: calibrated dose of emulsified vitamin D drops
Drink 1.5 litres of water a day with additional vitamin C, sulphur and potassium.
NAC as a liver booster
Iron supplementation
Niacinamide to calm acne lesion inflammation
Minerals and vitamins: including high dose B vitamins, and zinc, selenium, molybdenum, copper, manganese, chromium and boron
Active DIM to increase oestrogen detoxification
Saw palmetto complex to reduce testosterone levels
SYMPTOM TRACKING
Symptom
Score out of 6
Initial score
Acne There are massive cysts on her face for 10 days before her period and she can still feel them after period. They are painful when sleeps and wears glasses. She won’t go out if has cysts on her face.
5
Number of cysts
6
Mood disturbance Premenstrual anger, explosive irritability and crying.
6
Results – follow-up 1 (+4 weeks)
No acne – for the first time since she was 13 (and now is 33 years old)
Irritability drastically reduced, only had a few moments of feeling annoyed
No period pain
No flooding, normal menstrual flow.
No pain with ovulation
She struggled a bit with the required nutritional changes, especially with adding vegetables to every meal, but has now made it part of her usual diet.
SYMPTOM TRACKING
Symptom
Score out of 6
Initial score
Score after 4 weeks
Acne
5
0
Number of cysts
6
0
Mood disturbance
6
2
I’m really happy with what Sandra has done for me. My skin and mood have completely transformed, to the point where I am so happy.
BA
My review
I was delighted with the quick response that BA had to the protocol, and particularly with how happy and confident she became in her life.
Acne and PMS are so incredibly responsive to focused nutritional interventions, and BA ‘s experience is a perfect example of how having the know-how to balance hormones leads to such a positive results.
Reversal of chronic and severe daily premenstrual anxiety and depression that started in childhood in a 33 year old woman.
Overview
Many women experience premenstrual anxiety and depression in a moderate or severe form. Typically these are hormonal imbalances which are driven by nutrient deficiency and/or excess, which when resolved can lead to calm, uneventful, natural cycles.
Introduction
OT was 33 years when she got in touch with me seeking help for her long-standing daily anxiety and depression, which became much worse before her period. She felt low 80% of the time and even worse in the week before her period, where she would have an emotional meltdown. She had tried all kinds of approaches to manage her low moods including counselling, anti-depressants and hormonal birth control, none of which were successful.
She said:
“I have suffered with anxiety and low grade depression for as long as I can remember although I only realised that there was a name for how I felt when I was in my late teens. Whilst at college, I hit my lowest point and had some counselling but I think i only had a few sessions. The counselling did not work for me as it felt very “standardised” rather than looking to help me work through my own personal issues. I struggled with my mental health all through university but managed to distract myself with friends and work.
Recently I made positive changes to my diet, but I still suffer with anxiety and depression. I started taking sertraline as I again hit rock bottom. I stopped taking sertraline around 8-12 months ago as I was having bad side effects including severe night sweats. My anxiety and depression is also heightened a week leading up to my period and I am now looking for a more natural way to manage my symptoms as I hate how I feel most of the time. This state of being can be so frustrating at times as I know that I am very fortunate in my life but my mood is always low.
I believe my menstrual cycle has an effect as I have a few days around the time I am ovulating where I feel “normal” or better than I usually do.”
Health history
Gynaelogical:
regular cycles every 28-29 days
severe premenstrual anxiety, irritability, crying spells, mood swings, depression and lethargy
premenstrual food cravings, fatigue, headaches and breast tenderness
periods are light
periods last 2-3 days,
feels much better once period has ended for the next 3-4 days
then mood goes back to baseline, low but functional
mood better around ovulation
vaginal dryness
Digestive:
stomach upset by greasy foods
cravings for fat and meat before her period
Nutrition history
High carbohydrate breakfast e.g. apple and cinnamon porridge with oat milk
Low on protein
Low on vegetables
Low on fat
Has 3 meals a day but they are quite small
Test results
Vitamin D deficiency
Vitamin B12 deficiency
Folate deficiency
Low iron
Omega 6 too high
Omega 3 too low
Blood sugar too high
Root cause analysis
OT’s mood was low in general, which indicates a deficiency of serotonin and dopamine, and this was confirmed by a neurotransmitter questionnaire.
Depressive, anxious syndromes can be caused by nutritional deficiencies from poor diet, including
5HTP derived from animal protein which creates serotonin
tyrosine derived from animal protein which creates dopamine.
magnesium
calcium
Additionally, it was very clear that her low mood was cyclical, improving at ovulation when oestrogen is higher, and crashing premenstrually. It was also clear that her oestrogen was too low in general and progesterone was too high premenstrually, as evidenced by
light periods
short periods – 2-3 days
breast tenderness
vaginal dryness
Factors contributing to low oestrogen in OT included
inadequate fat intake: steroid hormones such as oestrogen (and vitamin D) are made from cholesterol which is derived from dietary fat, which she could not digest and absorb
inadequate B vitamins which prevents the synthesis of oestrogen from testosterone
Protocol
NUTRITION
I recommended a low carbohydrate, moderate protein, high fat nutrition plan which was rich in fish and eggs, with a high level of vegetables and beneficial fats, and personalised to OT’s requirements.
OT was asked to follow my 7 food rules as closely as possible.
SUPPLEMENTS
Vitamin D: calibrated dose of emulsified vitamin D drops
Gynovite: a multivitamin with high doses of B vitamins targeted for low oestrogen
5HTP to increase serotonin
L-tyrosine to increase dopamine
Body balance oil to increase fat intake
LIFESTYLE
I recommended that OT purchase a Seasonal Affective Disorder lamp and expose her eyes the bright light every morning. Bright light therapy has shown to help with winter blues, regulating energy in the daytime and the sleep cycle at night.
SYMPTOM TRACKING
Symptom
Score out of 6
Initial score
Daily depression
4
Daily anxiety
4
Depression before period
6
Anxiety before period
3-4
Meat cravings before period
5
Craving for fat before period
5
Results – follow-up 1 (+4 weeks)
4 weeks later OT, for the first time, did not have the usual pre-menstrual emotional meltdown of breaking down and crying, and was feeling emotionally well during the month.
She did have 2 short depressive episodes, but said that at the same time her workload was excessively stressful.
Her anxiety had improved slightly, and she was still finding it difficult to fall asleep.
Her skin had improved a lot.
Pre-menstrual fat and meat cravings had reduced.
She was enjoying eating more vegetables and protein, she wasn’t hungry between meals and most significantly she wasn’t having any mid-morning cravings for food.
The Gynovite supplement caused digestive issues so I switched it to Optivite PMT.
SYMPTOM TRACKING
Symptom
Score out of 6
Initial score
Score after 4 weeks
Daily depression
4
2
Daily anxiety
4
3
Depression before period
6
2
Anxiety before period
3-4
3
Meat cravings before period
5
2
Craving for fat before period
5
2
Results – follow-up 2 (+8 weeks)
4 weeks later and all of OT’s symptoms had resolved.
Again she had no breakdown before her period and her day-to-day emotional life was absolutely fine.
She had a couple of anxious moments related to work stress, but that was all.
All her cravings had gone. She was still having a little anxiety before sleep and I adjusted her protocol to help with that.
She was finding it difficult to stomach the oil so I switched the oil to capsules instead.
SYMPTOM TRACKING
Symptom
Score out of 6
Initial score
Score after 4 weeks
Score after 8 weeks
Daily depression
4
2
0
Daily anxiety
4
3
1
Depression before period
6
2
0
Anxiety before period
3-4
3
0
Meat cravings before period
5
2
0
Craving for fat before period
5
2
0
OT’s review
“Within weeks of starting my supplement plan, I noticed a significant positive shift in my mental health and I am confident that this will continue going forward.
I can honestly say that with Sandra’s help, my life has changed for the better.”
I have struggled with anxiety and depression for as long as I can remember. Having tried everything from counselling, antidepressants and even Reiki, I was beginning to feel as though I would have to live with my anxiety and depression forever.
I made contact with Sandra following a recommendation from a friend and I am so glad I did. During the initial call, Sandra made me feel at ease straight away.
Within weeks of starting my supplement plan, I noticed a significant positive shift in my mental health and I am confident that this will continue going forward. I can honestly say that with Sandra’s help, my life has changed for the better.
Thank you Sandra!
My review
Despite the fact that I see significant improvements in client’s health every day in my work, it still sometimes takes my breath away when I see the power of functional medicine in action.
I always expect to see results within 4 weeks, and OT’s progress was no different. She was committed to the process right from the start and did an incredible job of following her plan.
As she said to me, and I agreed – “I wish I could have done this years ago, and I dread to think what my life would have been like if I hadn’t done this work with you”. It saddens me to think of all the women that are suffering through their cycles and not getting the help they need, and I am so pleased to have seen OT recover so quickly.
Endometriosis is a chronic gynecologic disease process with multifactorial etiology. Increased oxidative stress, a result of increased production of free radicals or depletion of the body’s endogenous antioxidant defense, has been implicated in its pathogenesis. Oxidative stress is thought to promote angiogenesis and the growth and proliferation of endometriotic implants. Oxidative stress in the reproductive tract microenvironment is known to negatively affect sperm count and quality and may also arrest fertilized egg division leading to embryo death. Increased DNA damage in sperm, oocytes, and resultant embryos may account for the increase in miscarriages and fertilization and implantation failures seen in patients with endometriosis.
The evidence linking endometriosis and infertility to endogenous pro-oxidant imbalance provides a rationale for the empiric use of antioxidant therapy. Vitamin C and E deficiency has been demonstrated in women with endometriosis. Observational and randomized controlled studies have shown vitamin C and E combination therapy to decrease markers of oxidative stress.
Endometriosis is a painful condition of the female reproductive organs that can result in heavy bleeding, scarring, fatigue, infertility, and more.
A study published in April 2018 using data collected from 70,835 premenopausal women has examined if there is a connection between fruit and vegetable consumption and endometriosis. While there didn’t appear to be an association between total vegetable intake and risk of endometriosis, citrus fruits were associated with a lower risk of the disease. Based on data from food frequency questionnaires every four years between 1991 to 2013, women consuming ≥1 servings of citrus fruits per day had a 22% lower endometriosis risk compared to those consuming <1 serving per week.
The researchers concluded, “Our findings suggest that a higher intake of fruits, particularly citrus fruits, is associated with a lower risk of endometriosis, and beta-cryptoxanthin in these foods may partially explain this association.”
As search for optimal therapy continues for endometriosis, aid of dietary supplements is gaining attention. Supplements can be used for their anti-inflammatory, anti-oxidant, anti-proliferative and immune modulatory characteristics. We reviewed the literature, evaluated and synthesized effects of vitamin D, zinc, magnesium, omega 3, propolis, quercetin, curcumin, N-acetylcysteine, probiotics, resveratrol, alpha lipoic acid, vitamin C, vitamin E, selenium and epigallocatechin-3-gallate. Based on results of in vitro, animal and human studies, it might be safe to say that dietary supplements can be used as a complementary treatment for endometriosis.
Endometriosis is a common chronic inflammation causing major problems including infertility. The role of omega-3 and omega-6 fatty acids as their potential anti-inflammatory effects in endometriosis needs to be further explored. The objective of this study was to compare serum phospholipid fatty acid profile in endometriosis patients with controls, and to explore the correlation of this profile with the severity of the disease.
Methods:
Sixty-four endometriosis patients and 74 control women, in reproductive age, participated in this study. Among the endometriosis patients, 19 cases were in stage I, 27 cases in stage II, 8 cases in stage III, and 10 cases in stage IV. Each patient underwent laparoscopy. Before surgery, 5 ml of blood was obtained. After extraction of the total lipids, serum total phospholipid fraction was isolated by thin layer chromatography. Fatty acid composition of the phospholipid fraction was determined by gas chromatography and the resulted profile was compared in endometriosis patients and controls. The profile was also compared in the endometriosis group based on the severity of disease.
Results:
Stearic acid was significantly lower in the endometriosis group as compared to controls (P= 0.030). No other fatty acid compositions were significantly different between patients and controls. Serum ratio of eicosapentaenoic acid (EPA) to arachidonic acid (AA) was in reasonable correlation with the severity of endometriosis (r = 0.34, P = 0.006).
Conclusion:
According to these findings, levels of fatty acids in serum total phospholipids seem not to be a marker for endometriosis, but the EPA to AA ratio was a relevant factor indicating severity of illness.
EPA is hypothesized to reduce disease severity through their anti-inflammatory and immunomodulatory effects [25]. EPA is the most important component of omega-3 and AA, an omega-6 fatty acid and plays an important role in biological systems. AA has a substrate role for production of certain mediators such as PGE2 and leukotriene (LTB4). PGE2 and LTB4 are initiators for endometriosis and pain [24]. On the other hand, EPA plays a role in biosynthesis of LTB5 and PGE3 which have less inflammatory effect compared with PGE2 and LTB4 [24]. EPA is a competitive inhibitor in conversion of AA to LTB4 and PGE2 [26]. Irrespective of study design, our results were in agreement, in part, with the in vitro experiments by Gazvani et al. [20] that showed a high ratio of omega-3 to omega-6 in endometrial cell culture from endometriosis patients induce higher concentrations of IL-8 productions in cell supernatant. IL-8 as a pro-inflammatory and angiogenic cytokine has a significant role in endometriosis [27].
Floating around the internet in recent weeks was an announcement from Argentinian researchers who, quite by accident, found that sterile women’s health products were anything but sterile.
It turns out that cotton grown from genetically modified cotton seeds and sprayed with glyphosate (RoundUp and other herbicides) across the growth cycle, retain, and likely leach, glyphosate from the products that the cotton is spun into. It should not be a surprise that those cotton-based products retain the chemicals from which they were grown or processed, but it was. Not because the idea is far-fetched, it isn’t. Indeed, it is biologically more likely that these chemicals are retained than it is that they somehow would magically disappear post processing. What was surprising is that we never thought about this before.
When we consider that 89% of cotton crops are now genetically modified to be glyphosate tolerant, the implications of glyphosate transfer from what are considered sterile medical and hygiene products directly into the bloodstream of the users should give us pause. Heck, it should have given us pause many years ago, but it didn’t and wouldn’t yet if it were not for some accidental finding in a lab studying something else entirely. This accident speaks volumes about how thoroughly we test, or rather, do not test, many of the products we have on the market. It is precisely this lack of testing and lack of understanding that leads to the preponderance of chronic health conditions from which so many in the Western world suffer.
Glyphosate and Women’s Health
If we look at women’s health in particular, I cannot help but wondering if glyphosate leaching tampons have something to do with the increase in menstrual related problems like fibroids, endometriosis, PCOS, and others. The female vagina and cervix are remarkably efficient vehicles for drug absorption. The vaginal epithelium provides a vast surface area that is richly vascularized and highly innervated. Drugs and other chemicals absorbed via this route directly enter the bloodstream and avoid detoxification via the liver, meaning lower dosages are required to reach the same effect as an orally ingested medication. Small concentrations, therefore, could induce large effects. And small, regular exposures to glyphosate is likely what we get from tampon use.
Infertility affects as many as 12.3% of women ages 15-44 (or 7.5 million women) in the United States.
Consequently, it is imperative to find methods to help women overcome infertility so that they may conceive a healthy child.
Many of the current treatments for infertility are costly, have low success rates, and have the potential to negatively affect long-term health. The common medical interventions used for infertility include fertility medications, in-vitro fertilization (IVF), and intrauterine insemination (IUI). Fertility medications, such as clomiphene and gonadotropins, stimulate growth of the ovarian follicle, followed by follicular rupture induced by a human chorionic gonadotropin (hCG) trigger shot.
These medications are often used in conjunction with IVF and IUI. IVF is an assisted reproductive technology that includes combining an egg and a sperm in a laboratory and then transferring the fertilized embryo into the uterus. IUI involves placing the sperm inside of the uterus to help with fertilization. Although less invasive and expensive than IVF, in IUI the sperm has to fertilize the egg on its own within the woman’s reproductive tract.
Research suggests a link between a variety of health conditions and subsequent infertility, including polycystic ovarian syndrome (PCOS), endometriosis, advanced maternal age (AMA), high body mass index (BMI), the MTHFR genetic mutation, hypothyroidism (both clinical and subclinical), and poor ovarian reserve.
In this article, we provide case evidence for alternative methods for managing infertility that are effective at improving the underlying condition leading to infertility – methods that are less expensive than medical intervention and are supportive of long-term health.
NAC (N-acetylcysteine) treatment or no treatment was offered to 92 consecutive Italian women referred to our university hospital with ultrasound confirmed diagnosis of ovarian endometriosis and scheduled to undergo laparoscopy 3 months later.
According to patients acceptance or refusal, NAC-treated and untreated groups finally comprised 73 and 72 endometriomas, respectively.
After 3 months, within NAC-treated patients cyst mean diameter was slightly reduced (−1.5 mm) versus a significant increase (+6.6 mm) in untreated patients (P = 0.001).
Particularly, during NAC treatment, more cysts reduced and fewer cysts increased their size.
Our results are better than those reported after hormonal treatments.
Twenty-four NAC-treated patients—versus 1 within controls—cancelled scheduled laparoscopy due to cysts decrease/disappearance and/or relevant pain reduction (21 cases) or pregnancy (1 case).
Eight pregnancies occurred in NAC-treated patients and 6 in untreated patients.
We can conclude that NAC actually represents a simple effective treatment for endometriosis, without side effects, and a suitable approach for women desiring a pregnancy
Supplementation with myo-inositol may be considered a reliable option in the treatment of metabolic syndrome in postmenopausal women.
The aim of this study was to evaluate whether myo-inositol, an insulin-sensitizing substance, may improve some features of metabolic syndrome in postmenopausal women.
Methods:
Eighty postmenopausal women affected by the metabolic syndrome were enrolled prospectively in the study and treated with diet plus supplementation of myo-inositol (2 g BID plus diet: intervention group) or with diet plus placebo (control group) for 6 months. They were evaluated at baseline and after 6 months for insulin resistance (homeostasis model assessment ratio [HOMA] insulin resistance), lipid profile, and blood pressure.
Results:
Myo-inositol plus diet improved systolic and diastolic blood pressure, HOMA index, cholesterol, and triglyceride serum levels with highly significant differences, compared with the groups treated only with diet and placebo. In the group treated with myo-inositol, a decrease in diastolic blood pressure (−11%), HOMA index (−75%), and serum triglycerides (−20%) and an improvement in high-density lipoprotein cholesterol (22%) were shown.
Conclusions:
Supplementation with myo-inositol may be considered a reliable option in the treatment of metabolic syndrome in postmenopausal women.
Polycystic ovary syndrome (PCOS) is a complex and common endocrine disorder characterized by hyperandrogenism, which is accompanied by follicle growth arrest at the small antral stage, minimal granulosa cell proliferation, and chronic anovulation.
Polyunsaturated fatty acids (PUFAs) are necessary for the body’s metabolism, growth and development. Although PUFAs play an important role in the regulation of female reproduction, their role in ovarian development in PCOS is still unclear.
The present study was conducted to investigate the effects of different ratios of n-3/n-6 PUFAs (omega-3/omega-6) on ovary development in PCOS rats. Serum levels of reproductive hormones and enzymes related to steroidogenesis were assessed.
The results indicated that PUFAs (n-3/n-6: 1/15) significantly increased ovarian weight and improved the ovarian structure although they had no significant effect on body weight in PCOS rats.
Meanwhile, apoptosis was attenuated accompanied by increased cell proliferation by PUFAs (n-3/n-6: 1/15). Moreover, serum levels of hormones (FSH and E2) were also significantly increased by PUFAs (n-3/n-6: 1/15) accompanied by decreased T levels.
To investigate whether PUFAs regulate the expression of enzymes related to hormone synthesis, western blotting was used to determine the protein levels of CYP51, CYP19, StAR and 3β-HSD.
The results showed that PUFAs significantly increased the protein levels of all of these enzymes. These results indicate that PUFAs enhance the reproductive performance of PCOS by increasing the expression of steroidogenesis enzymes, which are related to hormone secretion and ovarian functions.
These findings provide evidence that a balanced n-3/n-6 PUFA ratio is beneficial for PCOS reproduction.
There is now compelling evidence for a link between enteric microbiota and brain function. The ingestion of probiotics modulates the processing of information that is strongly linked to anxiety and depression, and influences the neuroendocrine stress response.
This study found that taking a prebiotic called galactooligosaccharides for three weeks significantly reduced the amount of cortisol, a primary stress hormone in the body.
Berberine inhibits the proliferation of human uterine fibroid cells
Treatment of fibroid cells with berberine inhibited cell proliferation by approximately 60%.
COX-2 is a critical enzyme that converts arachidonic acid into prostaglandin E2 (PGE2) and is commonly overexpressed in many solid tumors, including colorectal, breast, prostate, and ovarian neoplasms.
Increased expression of COX-2 and the associated PGE2 production have been demonstrated to significantly enhance carcinogenesis. Ke et al. reported that COX-2 expression was significantly up-regulated in uterine fibroids and that the inhibition of COX-2 activity significantly reduced the proliferation of the uterine fibroids smooth muscle cells, which suggests that COX-2 is involved in the pathogenesis of uterine fibroids.
In turn, berberine has been reported to induce cancer cell apoptosis and suppress cancer cell migration in many neoplastic cell lines, including melanoma, non–small cell lung cancer (40), and oral cancer, an effect mediated through the reduced expression of COX-2.
Consistent with these observations, our data indicate that BBR significantly reduced COX-2 expression in uterine cells, which suggests that COX-2 may also play a role in mediating BBR-induced apoptosis in human uterine cells.
Berberine inhibits the proliferation of human uterine fibroid cells
Metabolic syndrome is a cluster of conditions that occur together, including
increased blood pressure
high blood sugar
excess body fat around the waist, and
abnormal cholesterol or triglyceride levels.
Having just one of these conditions doesn’t mean you have metabolic syndrome but as you develop more of these conditions, your risk of complications such as type 2 diabetes and heart disease, rises higher and higher.
Research shows that the more carbohydrates you eat, the more likely you are to have metabolic syndrome:
for every 5% intake of energy from carbohydrates, the increase in the risk of metabolic syndrome goes up by 2.6%.
We tend to think that a loss of mental acuity is just part of getting older — but age is not the only contributing factor to cognitive decline. Our lifestyle also plays a key role. Failing to follow a nutritious diet, a lack of sleep and exercise, ongoing stress, smoking, drinking alcohol excessively and environmental pollutants can all damage our brain cells.
Fortunately, mental deterioration is not irreversible. In fact, the brain is incredibly dynamic and has the potential and the ability to change at any point throughout our entire life – and you have the power to enhance your brain function, protect your brain from damage and counteract the effects of aging! That is, if you’re willing to fuel the brain and tweak your everyday decisions.
Here are 5 small changes you can make in your life that can mean big differences in your cognitive abilities.
As women start to produce less estrogen and enter perimenopause, they are likely to experience a mix of challenging symptoms. These include hot flashes, insomnia, night sweats, vaginal dryness, and mood swings.
Menstrual periods may get lighter or heavier and less regular, but once a woman has not had a period for 12 months, they are in menopause. Then, the symptoms experienced over the previous years begin to subside.
There is a range of vitamins and supplements available to help women manage the symptoms of perimenopause and menopause.
If you feel as though you can’t do as much physically as you’ve gotten older, there may be a reason. Both aging and menopause are known to affect sarcopenia, which is a loss of muscle mass and strength, which in turn affects balance, gait, and overall ability to perform tasks of daily living. A new study is one of the first to link alcohol consumption with a higher prevalence of sarcopenia in postmenopausal women. The study outcomes are being published online today in Menopause, the journal of The North American Menopause Society (NAMS).
Previous studies of postmenopausal women have suggested the beneficial effect of estrogen therapy on muscle mass and function. Because of this, it is believed that postmenopausal women are more vulnerable to sarcopenia. Although alcohol is known to inhibit skeletal muscle protein synthesis, few studies have examined the relationship between sarcopenia and alcohol-drinking patterns.
…Study results published in the article “Associations between high-risk alcohol consumption and sarcopenia among postmenopausal women” show that the prevalence of sarcopenia was found to be nearly four times greater for the high-risk, alcohol-drinking group than the low-risk group.
…With this study suggesting that more muscle loss leads to sarcopenia and other studies suggesting that even one drink of alcohol may increase the risk of breast cancer, postmenopausal women should limit their alcohol intake.”
The therapeutic benefits of omega-3 fatty acids – which are abundant in certain fish oils – have long been known. In the 1950s, upon the discovery that omega-3 improves brain development, cod liver oil was given for free to young children, pregnant women, and nursing mothers. In the 80s, scientists reported that eskimos enjoy better coronary health than their mainland counterparts as a result of their fish rich diets. And in 2009, a study published in the Menopause journal suggested that omega-3 helps reduce the frequency of hot flushes in menopausal women.
As you can see, the hype that surround omega-3 is warranted, and not something to be shied away from.
The Truth About Fats
Many women are concerned about fat, and wrongly believe that consuming fat will make them overweight. The truth is, however, that an extremely low-fat diet won’t regulate your weight – and it certainly won’t enhance your health. Fat can be hugely beneficial in the right form, and by consuming fatty acids such as omega-3, you will surely be more healthy.
Research has confirmed that omega-3 fatty acids may have an excellent effect on impacting degenerative diseases, such as heart disease, rheumatoid arthritis, hypertension, Alzheimer’s disease, diabetes, and many more. As for menopause, omega-3 fatty acids contain anti-inflammatory properties shown to have a positive effect on many of the symptoms associated with “the change”.
What can omega-3 help with?
Because of its wonderful properties, omega-3 can greatly help women during menopause. It helps treat a range of menopausal symptoms, such as:
Hypertriglyceridemia– Postmenopausal women may have higher triglyceride concentrations than premenopausal women, exposing them to increased risk of coronary heart disease. As omega-3 offers a triglyceride-lowering effect, many practitioners recommend menopausal women obtain a bare minimum 1g/day as provided by your diet or supplementation.
Joint pain/menopause arthritis– Omega-3 fats can reduce inflammation, which may help relieve joint pain and stiffness related to menopause arthritis. Omega-3s work in a similar way as non-steroidal anti-inflammatory drugs (NSAIDs).
Menstrual pain – As part of your ovaries’ frustrating grand finale, perimenopausal women often experience strong menstrual pain and cramping. This pain is often caused by substances called prostaglandins, which come in both “good” and “bad” form. Menopause promotes the bad kind, while omega-3 fatty acids promote the good kind.
Depression– Women are twice as likely to suffer depression compared with men, and the risk is even greater following menopause. Irritability and sadness are common emotional symptoms of menopause, but omega-3 may effectively alleviate these symptoms. Omega-3s work to improve mood and restore structural integrity to brain cells that are critical in performing cognitive functions.
Osteoporosis– An increased intake of omega-3 acids increases bone mineral content and produces healthier, stronger bones. As menopause can increase a woman’s risk of developing osteoporosis due to a drop in oestrogen levels, omega-3 fatty acids should be an essential part of a menopausal diet.
Hot flushes– The frequency of hot flushes in women going through menopause can vary from as little as once a week to every 30 minutes. Some hot flushes last minutes, while others a mere few seconds. Studies have shown that while omega-3 may not affect the intensity of hot flushes, it can halve the frequency of hot flushes with the right dosage.
Vaginal dryness– Fatty acids help to lubricate the body in general, therefore helping with dryness of the vagina – a common symptom of menopause.
Brain imaging and gene analyses in twins reveal that white matter integrity is linked to an iron homeostasis gene.
Iron deficiency is a well-known cause of impaired cognitive, language, and motor development, but a report out today (January 9) in Proceedings of the National Academy of Sciences reveals that even in apparently healthy young adults, variations in iron levels correlate with variations in brain structure integrity.
“[The researchers] make a very interesting connection between the issue of iron metabolism and the integrity of white matter, more specifically myelin”—the cellular sheath that enwraps and insulates neuronal axons—said George Bartzokis of the University of California, Los Angeles, who was not involved in the study. “This would have been predicted by what is known about myelin, because it actually contains a lot of iron, so it is important that [they have] directly demonstrated this in humans with imaging.
More forgetful? Not thinking as clearly? Simple arithmetic coming more slowly? Worried that mental functions are worsening? Are the processes of ageing catching up? There is much that can be done to prevent worsening mental functioning and memory loss. For some, memory loss heralds the onset of dementia. Regardless of a person’s occupation or social environment, loss of memory is the most feared consequence of ageing…
…Specific nutritional interventions and nutritional supplements can help to detox and protect individual cells of the brain and nervous system.
Get notified about new editions
Subscribe to the Sunday Supplement
Connecting women, science and spirit, the Gynelogic Sunday Supplement delivers a bi-monthly dose of news, views and reviews, as seen through my lady lens.