Adenomyosis is characterised by a constant pain on the top of the uterus. Adenomyotic lesions are fundamentally wounds undergoing repeated tissue injury and repair, which progress to fibrosis, with ensuing greater tissue stiffness, results in impairing endometrial repair and eventually can cause heavy menstrual bleeding. Wounding may be caused by medical uterine procedures, imbalance vaginal microbiome leading to uterine infections and/or excess oestrogen causing strong muscle contractions.
Adenomyosis is a condition where the tissue that normally lines the inside of the uterus is found within the muscular layer of the uterus. It is common in women who are of childbearing age, and can develop at any age. The most common symptom of adenomyosis is unrelenting pain, throughout the cycle, on the top of the uterus. Severe period pain is common and there may be heavy bleeding.
Adenomyosis can occur alongside endometriosis. Although endometriosis can be found in about 1 in 10 women of reproductive age, it is impossible to know how many women are affected by adenomyosis. That is because diagnosis of adenomyosis is often difficult. The gold standard tool for diagnosing adenomyosis is by histopathological examination of a womb which has been removed by hysterectomy, which of course is not an option or preferred choice for everyone. In contrast, the gold standard tool for diagnosing endometriosis is a laparoscopy (keyhole surgery), which does not necessitate removal of any organ. Up to 1 in 5 women attending a gynaecology clinic with heavy periods, pelvic pain or infertility, were found to have evidence of adenomyosis on ultrasound scan.
Studies using imaging to diagnose adenomyosis have reported an association between adenomyosis and an increased risk of preterm birth, small for gestational age, and pre-eclampsia among pregnant women who conceive spontaneously. Among women undergoing in vitro fertilisation and intracytoplasmic sperm injection treatment, adenomyosis is associated with a reduced rate of pregnancy and live births as well as an increased risk of miscarriage.
1. Presentation and Diagnosis
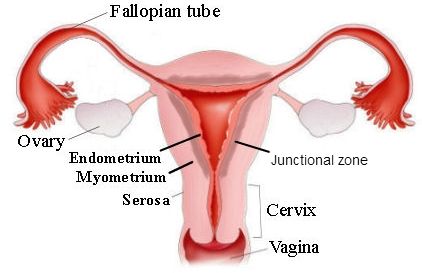
To understand adenomyosis, it is necessary to understand that the uterus has different layers. The innermost layer, which lines the uterine cavity, is called the endometrium. An embryo implants in the cells of the endometrium. The endometrium is what is shed each month when a woman has a period. Moving outward, the next layer is composed of mostly muscle and is called the myometrium. The myometrium can be further divided into an inner layer which is also called the junctional zone and an outer layer. The outermost layer of the uterus is a very thin covering called the serosa. In normal women, the “dividing line” between the endometrium and the junctional zone is clear and distinct and is thin.
In 80% of cases with histological adenomyosis (hysterectomy specimens), the junctional zone can be seen to be enlarged or thickened on an MRI scan:
less than 5mm thickening: normal uterus;
6-12mm thickening: diagnosis is unclear and could represent developing adenomyosis that not yet reaching diagnostic criteria. The test should be repeated within 12 months;
more than 12mm: proven adenomyosis.
Another important clue to the diagnosis of adenomyosis, especially in the younger (smaller) uterus, is the ratio of the junctional zone to the myometrium. In the absence of adenomyosis this ratio is less than .4 (40%). Greater than 40% is usually, but not always, also found where the junctional zone thickness is more than 12mm.
In teenage girls with adenomyosis the uterus is not yet matured, so if their junctional zone is in the 5 to 12mm range (strictly not diagnostic), but the ratio of the junctional zone to the myometrium is greater than 40% (in a small uterus), they should be treated as if they have adenomyosis.
This is particularly important where symptoms of endometriosis have led to a laparoscopy but no endometriosis was found. It is usually the case that adenomyosis is present.
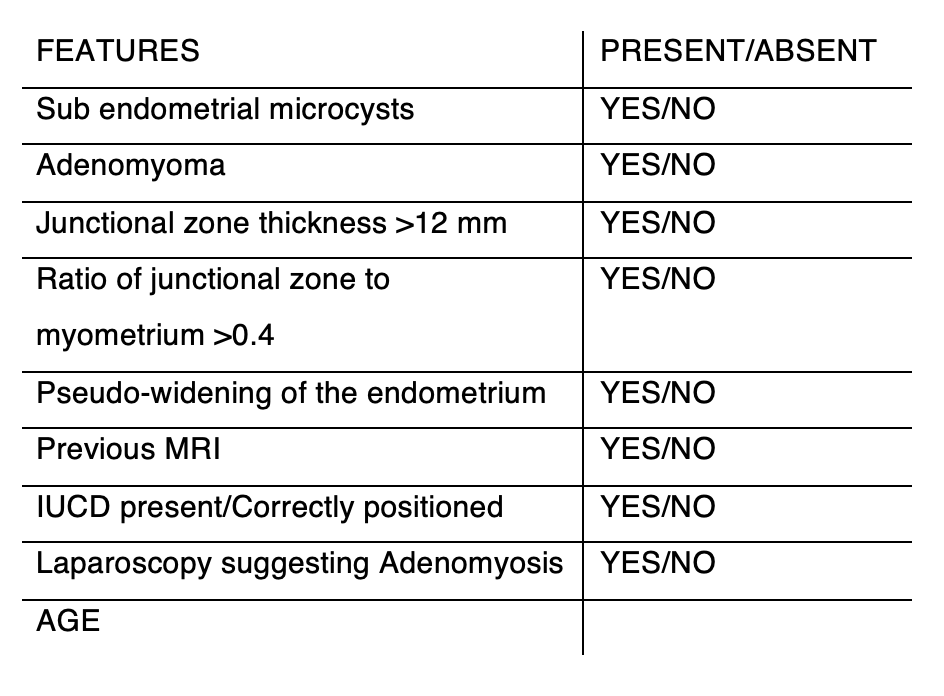
Dr Tronc uses this diagnostic table to identify adenomyosis, specifically whether the junctional zone is more than 12mm and whether there is an associated increase in the percentage thickness of the junctional zone amongst other features.
Dr Tronc reports that his choice of scanning techniques for the confirmation of adenomyosis is the MRI scan, not the ultrasound scan, because unless the radiologist is experienced in the diagnosis of early adenomyosis, an ultrasound scan may not give adequate results. In order to get the most accurate diagnosis, women should have the test performed in the “late proliferative” phase, usually on days 10 to 13 of a 28 day cycle. If someone is on the oral contraceptive pill, it seems not to matter when it is done.
Fibrosis is one important feature of adenomyosis. Elastography is a relatively new type of imaging technology that has become available for commercial use. It works by creating images that show how stiff different tissues are. There are two main types: ultrasound elastography (UE) and magnetic resonance elastography (MRE). Ultrasound elastography uses sound waves, while magnetic resonance elastography uses magnetic fields and radio waves.
This technology is similar to the traditional method of feeling for lumps or hardness in a clinical exam (palpation) but offers several advantages. Elastography is less subjective, meaning it doesn’t rely as much on the individual judgment of the clinician. It also doesn’t require as much experience to use, and it provides more precise information about where in the body the stiffness is located.
As of now, the use of MRE in the field of gynecology has been limited. However, ultrasound elastography is becoming more popular in this field. One of the biggest benefits of elastography is that it can detect a wider range of tissue stiffness in adenomyosis compared to other imaging methods like CT scans, standard ultrasounds, and MRI scans.
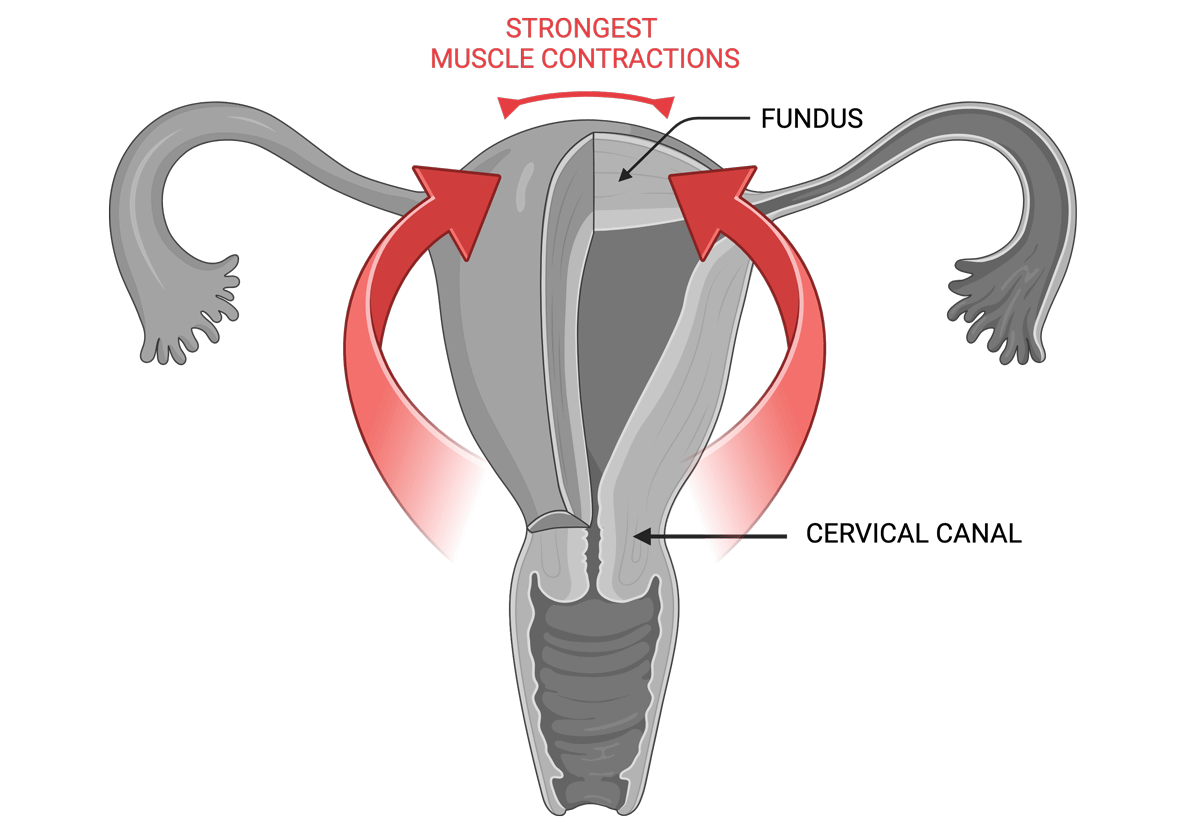
Early adenomyosis usually evolves in the central part of the fundus in the uterus. Even in more advanced cases of adenomyosis the expansion of the junctional zone in MRI often shows concentration of lesions at this location. During menstruation the muscular waves of contraction start in the cervical canal and rapidly move in the fundal direction, exerting their strongest power at the upper level of the uterus, which is where the most trauma will then occur, causing the intense pain of adenomyosis.
2. Development and Maintenance of Adenomyosis
The most comprehensive theory of of the development of adenomyosis involves the traumatisation of the uterine tissue followed by the initiation of the mechanism of tissue injury and repair (TIAR).
Injury resulting EMID leads to platelet aggregation, inflammation, and hypoxia (low oxygen), causing the release of copious inflammatory cytokines such as IL-1β and growth factors such as TGF-β1, increased local oestrogen production, as well as nerve damage.
Local oestrogen production
Oestrogen is critical to tissue repair, however it can disrupt the normal control that the ovaries have over the uterine muscle movements. As a result, the uterus starts to contract more frequently and intensely than usual, a condition known as hyperperistalsis. This excessive muscular activity can further harm the uterus, creating a cycle where the condition keeps getting worse on its own. Essentially, the ongoing damage leads to more inflammation and hormonal imbalances, which then causes even more damage, continuing the cycle of the disease.
Estradiol’s repair effects are primarily executed through the estrogen receptor-beta (ER2). Research, including animal experiments and studies on various body tissues like astroglia, bladder tissue, fibroblasts, and cartilage, has shown that healing after tissue injury involves locally produced oestrogen.
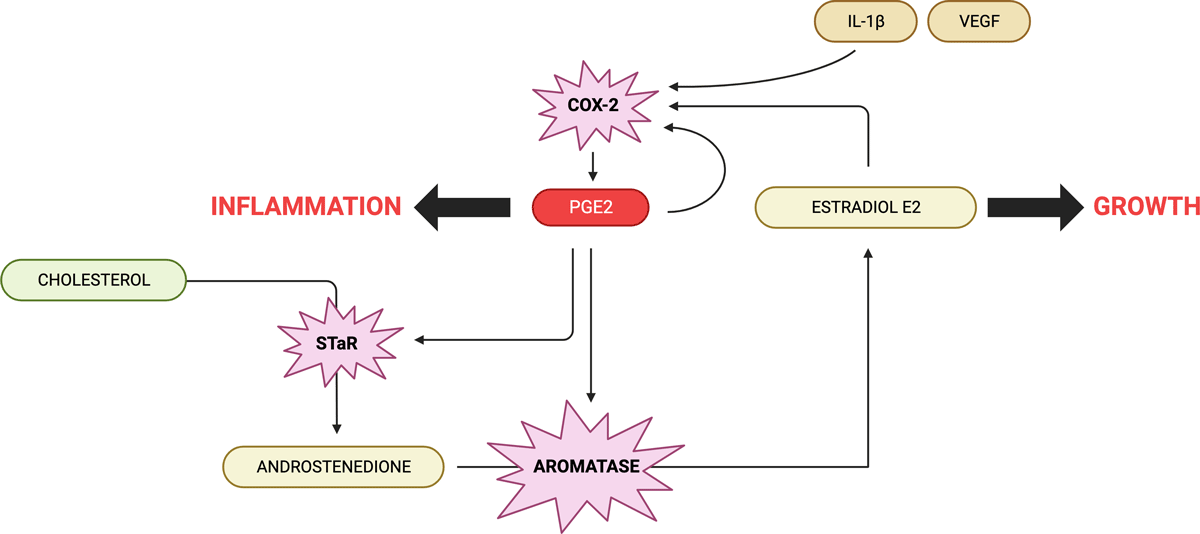
When tissue is injured, a substance called interleukin-1 activates the cyclooxygenase-2 (COX-2) enzyme, leading to the production of prostaglandin E2 (PGE2). PGE2 then activates the steroidogenic acute regulatory protein (STAR) and the P450 aromatase enzyme. This process facilitates the movement of cholesterol to the inner mitochondrial membrane, where testosterone is produced and subsequently converted into estradiol.
Intriguingly, studies with fibroblasts have shown that even minor physical strain can initiate this healing process.
The similarity of the molecular biology of TIAR in various tissues with that described in endometriosis strongly suggests that this represents the common underlying mechanisms of both diseases.
Additionally, the normal endometrial tissue can promote the growth of both nerves and blood vessels (neuroangiogenesis) through the release of tiny particles called exosomes. This increased nerve presence in the endometrium and the muscle layer of the uterus (myometrium) makes these areas highly sensitive. Therefore, even minor pain signals, changes in pain mediators, or abnormal muscle movements in the uterus can be significantly amplified. These signals are transmitted from the nerves in the uterus to the spinal cord and then to the brain, leading to the perception of pain. The situation is further worsened by the loss of GABAergic inhibition in the nervous system, a mechanism that usually blocks the transfer of pain signals to the brain.
Moreover, with more nerve fibers, especially an elevated density of sensory nerve fibers, there is an increase in the secretion of neuropeptides. However, some neuropeptides, such as substance P and calcitonin gene-related peptide (CGRP), can trigger changes in the ectopic endometrial cells that accelerate the formation of fibrous tissue (fibrosis) in the lesions.
In essence, the interplay of ectopic endometrial cells, increased nerve fibers, and altered neuropeptide levels in adenomyosis synergistically contribute to the pain experienced by women with this condition. This complex interaction involves nerve growth, heightened pain signal transmission, and tissue alterations in the uterus.
Heavy menstrual bleeding, lower PEG2?
In adenomyosis, the tissue becomes stiffer and more fibrous, leading to a decrease in COX-2 activity and lower PGE2 production. The reduction in PGE2 levels disrupts the hypoxia in the endometrium, impairing its ability to repair itself, which contributes to heavy menstrual bleeding. Studies have found that women with adenomyosis who experience heavy menstrual bleeding tend to have greater fibrosis in their lesions, accompanied by lower levels of HIF-1α, COX-2, and other related substances, indicating disrupted prostaglandin signalling and impaired endometrial repair.
Additionally, glycolysis, a process where glucose is broken down to produce energy, plays a crucial role in endometrial repair. The endometrium shifts to glycolysis during repair to meet increased energy demands and reduce oxidative stress, which can damage cells and tissues. However, reduced hypoxia signaling in fibrotic adenomyotic lesions, as seen in decreased levels of HIF-1α, can impair glycolysis. This impairment further disrupts endometrial repair, contributing to heavy menstrual bleeding in adenomyosis.
These findings provide a good explanation as to why different subtypes of adenomyosis have different symptoms. An early study indicated that adenomyosis lesions that penetrate less deeply into the myometrium, the muscular layer of the uterus, are more likely to be associated with heavy menstrual bleeding. This is because lesions closer to the lining of the uterus can more easily affect this area due to their physical proximity, thereby increasing the likelihood of heavy menstrual bleeding as the lesions progress. Additionally, internal adenomyosis, where lesions are within the muscle layer of the uterus, is commonly linked with heavy menstrual bleeding, whereas external adenomyosis, with lesions on the outer part of the uterus, often correlates with deep endometriosis and associated pain.
Heavy menstrual bleeding might further worsen the impairment of endometrial repair. The bleeding could lead to an accumulation of iron in the local area, potentially reducing the growth of endometrial stromal cells by inducing autophagy, a process where cells break down their own components. This could further hinder the endometrium’s ability to repair itself.
A vicious cycle of adenomyosis–pain–stress–lesional progression–more pain
Pain, heavy menstrual bleeding, and infertility can trigger various degrees of anxiety, discomfort, depression, and stress. When stress is chronic or persistent, it activates the Hypothalamic-Pituitary-Adrenal and Sympathetic-Adrenomedullary axes in the body, leading to the release of hormones called catecholamines, including adrenaline and noradrenaline. These hormones act on specific receptors and proteins in the ectopic endometrium (uterine lining cells found outside the uterus), notably adrenergic β2 and cAMP-responsive element-binding protein, accelerating the progression of lesions associated with the condition.
Chronic stress can also diminish the presence of dopamine receptor D2 in the ectopic endometrium. Dopamine is a neurotransmitter involved in mood regulation and other bodily functions. In contrast, positive stress, known as eustress, increases DRD2 presence in the lesions and slows their progression. This finding is consistent with research showing that dopamine or drugs activating DRD2 can hinder stress-related increases in blood vessel formation and cell growth in cancers.
Low dopamine levels can increase prolactin, a hormone important in the reproductive system. High prolactin can disrupt the secretion of gonadotropin-releasing hormone (GnRH), essential for reproductive health, leading to decreased levels of luteinizing hormone and follicle-stimulating hormone, affecting hormone production and fertility.
In mouse studies, implanting part of the pituitary gland (which produces prolactin) into the uterus induced adenomyosis. Also, higher prolactin levels in the bloodstream were associated with increased adenomyosis incidence. This evidence points to prolactin’s potential role in triggering adenomyosis. Treatment with bromocriptine, a dopamine agonist that reduces prolactin, completely halted adenomyosis development in some studies.
Another aspect of prolactin’s impact is its role in angiogenesis, the formation of new blood vessels. Vascular endothelial growth factor (VEGF) promotes angiogenesis. Dopamine agonists, like cabergoline, hinder VEGF from binding to its receptor on blood vessel cells, thus reducing angiogenesis. Animal studies on endometriosis showed that cabergoline treatment significantly decreased endometriotic lesion size and activity and VEGF production.
A self-perpetuating cycle emerges in adenomyosis, where the condition leads to pain and stress, which then accelerates lesion progression, resulting in more pain. This cycle highlights the intricate interplay between emotional and physical stress and the biological processes in adenomyosis, exacerbating the disease through a combination of hormonal and neurotransmitter effects.
3. My approach to resolving Adenomyosis
Nutrition:
Avoiding gluten, dairy, alcohol, soy and sugar can make a significant difference to reducing pain and inflammation
Supplements:
Vitamin E has been shown to prevent adenomyosis in a study that used Fluoxetine to induce it. Fluoxetine is an antidepressant from SSRI group having effect on reproductive organs by increasing oxidative stress. Administering vitamin E to fluoxetine-induced adenomyosis prevented the rise of prolactin and the development of adenomyosis.
L-tyrosine increases the production of dopamine and can reduce uterine pain.
L-arginine can prevent hypoxia and reduce uterine pain and heavy bleeding.
Agnus castus can reduce prolactin.
DIM and Myomin can improve the overall balance of oestrogens.
Quercetin can inhibit the proliferation of ectopic endometrial stromal cells in adenomyosis and reduce their mobility and invasiveness.
Adenomyosis is characterised by a constant pain on the top of the uterus.
Adenomyotic lesions are fundamentally wounds undergoing repeated tissue injury and repair, which progress to fibrosis, with ensuing greater tissue stiffness, resulting in impaired endometrial repair and eventually causing heavy menstrual bleeding.
Wounding may be caused by medical uterine procedures, imbalance vaginal microbiome leading to uterine infections and/or excess oestrogen causing strong muscle contractions.
A high level of prolactin can induce adenomyosis.
Adenomyosis can be managed by avoiding gluten, dairy, alcohol, soy and sugar.
Helpful supplements include vitamin E, l-tyrosine, l-arginine, Agnus castus, DIM, Myomin and quercetin.
Endometriosis most likely starts with differentiation and migration of Mullerian tissue during the formation of the embryo resulting in patches of this tissue being laid down in abnormal locations in the pelvis or elsewhere in the body. Later in life, these misplaced patches of tissue develop into endometriosis when they are exposed to oestrogen. The maintenance of endometriosis is largely mediated by prostaglandin E2 which leads to increased growth of lesion, inflammation and pain.
Endometriosis is a complex and often misunderstood condition that affects millions of women worldwide. It occurs when the tissue similar to the lining of the uterus, known as the endometrium, grows outside the uterus. This misplaced tissue can be found in various areas of the body, such as the ovaries, fallopian tubes, pelvic lining, and even distant organs like the bladder or intestines.
Unlike the normal endometrial tissue that sheds during menstruation, the displaced endometrial tissue has no means of exit from the body. This can lead to the formation of painful adhesions, scar tissue, and the development of cysts, causing a range of symptoms and complications.
1. Early warning signs
It is often difficult to evaluate endometriosis by physical examination and clinical history review. The warning signs include:
The first sign is unbearable period pain from the very first period. The typical symptoms in teenage girls include:
Avoidance of exercise during the period, particularly if due to excessive pain or heavy flow
Increased anxiety, depression and/or fatigue in relation to pain
Nausea with pelvic pain, especially if it is non-cyclic pain
Period pain or pelvic pain so severe it interferes with school/socialising/work/daily activities
Gastrointestinal problems such as diarrhoea/constipation particularly around the time of the period and in relation to period pain
Pelvic pain/period pain that does not respond to treatment with painkillers or hormonal treatments like the pill
Heavy or irregular periods
Pain during intercourse
Digestive problems – the endo belly – pronounced bloating or swelling of the abdomen, which can often be uncomfortable or painful, often accompanied by a feeling of ‘fullness’ in the abdomen. This bloating may occur at certain points of the menstrual cycle or randomly at other points of the month.
One of the common symptoms of endometriosis is very painful bowel movements specially during the menstrual cycle. But the bowel symptoms are not only limited to painful defecation, but it can include the following:
Constipation
Diarrhea
Bloating
Rectal bleeding
Nausea and vomiting
Infertility and furthermore, studies on IVF have shown that women with endometriosis have higher rates of pregnancy loss, complication of preterm delivery, pre-eclampsia and infants small for gestational age.
2. Presentation and Diagnosis
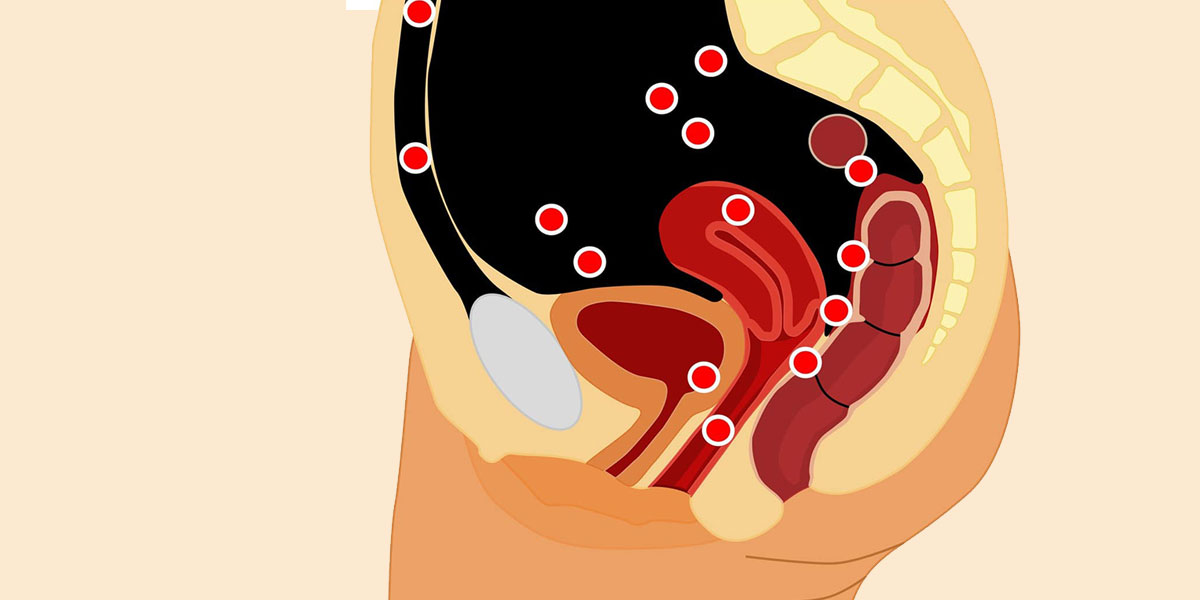
Endometriosis most often occurs on or around reproductive organs in the pelvis or abdomen, including:
Fallopian tubes
Ligaments around the uterus (uterosacral ligaments)
Lining of the pelvic cavity
Ovaries
Outside surface of the uterus
Space between the uterus and the rectum or bladder
More rarely, it can also grow on and around the:
Bladder
Cervix
Intestines
Rectum
Stomach (abdomen)
Vagina or vulva
Endometrial tissue growing in these areas does not shed during a menstrual cycle like healthy endometrial tissue inside the uterus does. The buildup of abnormal tissue outside the uterus can lead to inflammation, scarring and painful cysts. It can also lead to adhesions – the buildup of fibrous tissues between reproductive organs that causes them to “stick” together.
Diagnosing endometriosis requires a combination of medical history, physical examination, and imaging tests such as ultrasound or MRI. A definitive diagnosis can only be made through laparoscopy, a surgical procedure in which a thin tube with a camera is inserted through a small incision in the abdomen to view the pelvic organs and remove any abnormal tissue for biopsy.
Some of the procedures to diagnose a suspected case of endometriosis are
Laparoscopy: It is a surgical process. A camera is utilized to have a look into the abdominal cavity and estimate the severity of the condition. It visualizes the externally visible lesions. If the lesions are not visible, a biopsy can be drawn. This process of diagnosis also allows for surgical treatment through laparoscopy. 6 to 13 percent of women have shown the invisible lesions of endometriosis in the biopsy.
Ultrasound: a pelvic ultrasound detects the larger endometriotic cysts as in ovaries called endometriomas. However, it has no role in diagnosing smaller implants. Vaginal ultrasound is used in detecting deeper endometriomas and before operating on them. This is one of the most easily accessible, inexpensive and required no preparation.
Magnetic resonance imaging: it is a noninvasive technique. But due to its limited availability and cost, it is not widely recommended. But it precisely and accurately diagnoses smaller lesions.
Diagnosis delays – it’s something else
A US survey found that 75.2% of endometriosis sufferers were initially misdiagnosed as either having another physical disorder or mental health issue and many doctors choose to go down the route of symptom management like pain relief or hormonal medication without any formal diagnosis.
Why is there such a delay in the diagnosis of endometriosis? Studies have found that women are less likely to feel listened to and taken seriously, and are assumed to have a higher pain threshold. One of the main side effects of endometriosis is chronic pain, and because endometriosis patients don’t receive a definitive diagnosis until they’ve had laparoscopic surgery, not having their pain believed can be particularly harmful.
Activists have used the term ‘gender health gap’ to bring together evidence that would suggest that your gender has a bearing on your experience with doctors and the healthcare you receive. Studies that point out that women are 25% less likely than men to receive pain relief have been used to back up the notion of gender bias in medicine.
In a study published in 2018, entitled “Brave Men” and “Emotional Women”, researchers concluded that pain experienced by women was often described as medically inexplicable, as there was often no visible cause for their pain. As a result, healthcare professionals often attributed the pain to a psychological rather than physical cause. This was due to the absence of any visible or diagnostic evidence of illness.
The gender health gap, especially as it relates to endometriosis, has historical roots in medical practice. Endometriosis.org explains that pain associated with endometriosis is often dismissed because “‘women’s problems’ perplexed nineteenth-century doctors, who saw them as indicative of unstable and delicate psychological constitutions. Even though attitudes […] have improved during the twentieth century, some of the old beliefs still linger unconsciously, and affect the medical profession’s attitudes towards complaints including period pain.”
In 2014, Brigham and Women’s hospital in the U.S. said that medical developments that look into the way conditions are treated and diagnosed “routinely fail to consider the crucial impact of sex and gender. This happens in the earliest stages of research when females are excluded from animal and human studies or the sex of the animals isn’t stated in the published results.” This would suggest that in order to tackle the gender health gap and improve medical understanding of conditions like endometriosis, medical research that includes and prioritizes the experiences of people who identify as women need to take place in higher numbers.
The lack of medical research on endometriosis leads to less medical education on the disease, and can result in serious delays in the period of time it takes to receive an endometriosis diagnosis and how much your doctors understand about the condition.
Misdiagnoses
Many women with endometriosis who have gastrointestinal symptoms are often misdiagnosed as
Inflammatory bowel disease
Crohn’s disease
Appendicitis
If symptoms are cyclical in nature, it’s a sign indicating endometriosis. Some women may have symptoms throughout the cycle in chronic cases but the symptoms do aggravate during menstruation
3. Origin of Endometriosis
The origin of endometriosis is still not well defined. Many hypotheses have been proposed to explain the development of endometriosis and Dr David Redwine has proposed the most viable theory – Mulleriosis – that appears to cover all the salient features of endometriosis. His theory favours a genetically-driven embryonic origin of endometriosis. Müllerian tissue is tissue in a female embryo that eventually develops into the fallopian tubes, uterus, cervix and the upper part of the vagina. Mulleriosis indicates a problem of differentiation and migration of any Mullerian tissue during the formation of the embryo which results in patches of this tissue being laid down in abnormal locations in the pelvis or elsewhere in the body. Later in life, these misplaced patches of tissue develop into endometriosis when they are exposed to oestrogen.
To support his theory, Dr Redwine described a case of fingertip endometriosis, where surgical excision brought complete relief. He posits that that’s because the entire tract of Mulleriotic tissue that had been laid down in the dermis or nail bed had been removed by excision.
Via Dr David Redwine:
The cause of endometriosis is a subject of continued debate. My best guess is that it is a disease that the woman is born with because of a process called embryologically patterned metaplasia. At the moment of conception, a woman is dealt three cards.
The first card is that she will have endometriosis.
The second card is where in her body the disease will be.
The third card is how biologically active the disease will be in each area.
And depending on these various cards, which can be quite different from patient to patient, endometriosis, or areas that will become endometriosis, are laid down in the woman’s pelvis or elsewhere in the body during foetal formation. When oestrogen production begins at puberty, the tracts of tissue that were laid down can become painful and can begin to change into endometriosis. Men can also develop endometriosis for somewhat the same reasons.
Excision is the only cure
Going by Dr Redwine’s theory, excision of the lesions is the only cure for endometriosis, however it needs to be done by a surgeon who is specialised at removing the lesions ‘from the root’ otherwise they will grow back. The recurrence of endometriosis after ovarian endometrioma excision has been evaluated at 24, 36, 60, and 120 months as 5.8%, 8.7%, 15.5% and 37.6% respectively.
4. Development and Progression of Endometriosis
Endometriosis is driven by oestrogen that may come from the ovaries or from within the lesions themselves. Women with endometriosis tend to to have higher ovarian production of oestrogen and this combined with lesional oestrogen can result in high levels that make symptoms worse.
The central driver connecting oestrogen to symptoms is the high production of prostaglandin E2 (PGE2). PGE2 is a regulator that makes the environment inside the body more favourable for endometriosis to develop and progress by affecting various cellular activities and immune responses. Specifically, it:
Promotes cell growth (cell proliferation): PGE2 makes cells multiply faster, which can contribute to the growth of endometrial tissue where it shouldn’t be.
Prevents programmed cell death (antiapoptosis): Normally, cells have a built-in process of dying when they are damaged or not needed, called apoptosis. PGE2 stops this process, allowing potentially harmful cells to survive longer.
Weakens the immune system’s response (immune suppression): It hinders the body’s immune system from effectively responding to these abnormal cells.
Stimulates the formation of new blood vessels (angiogenesis): PGE2 encourages the growth of new blood vessels, which can supply more nutrients to the endometrial tissue growing outside the uterus, allowing it to grow more.
Feedback loop between oestrogen and PGE2 promotes growth and inflammation
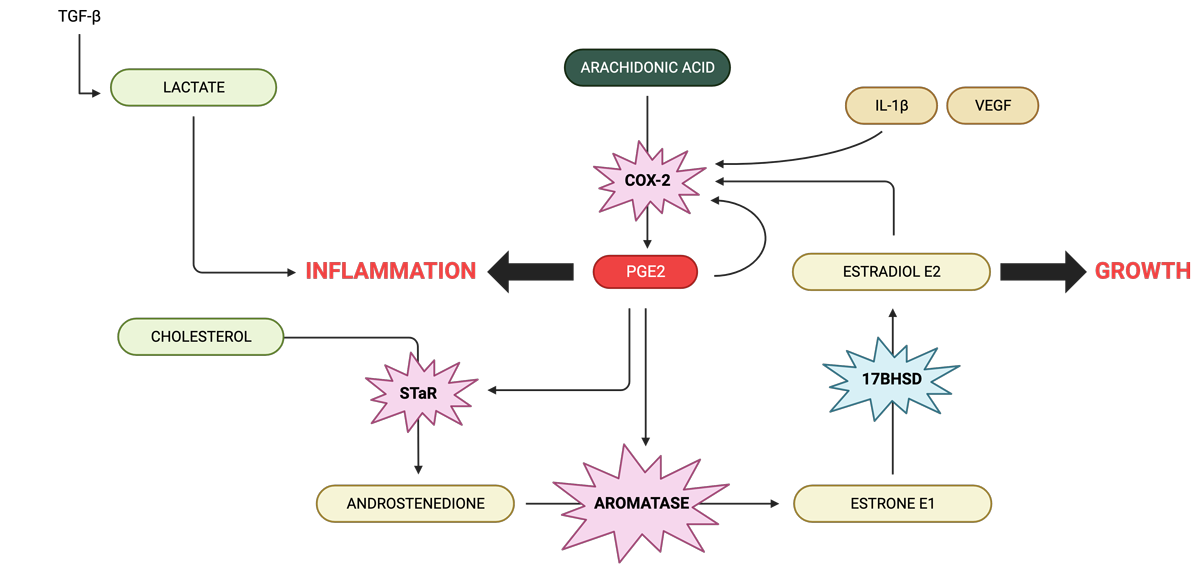
Two basic pathologic processes, namely growth and inflammation, are responsible for chronic pelvic pain and infertility, which are the primary devastating symptoms of endometriosis. Estrogen enhances the growth and invasion of endometriotic tissue, whereas PGE2 and cytokines mediate pain, inflammation and infertility.
Estradiol (E2) is produced locally in endometriotic tissue. The precursor, androstenedione of ovarian, adrenal or local origin becomes converted to estrone (E1) that is in turn reduced to E2 in endometriotic implants.
Endometriotic tissue is capable of synthesising androstenedione from cholesterol via the activity of steroidogenic acute regulatory protein (StAR) and other steroidogenic enzymes also present in this tissue. E2 directly induces cyclo-oxygenase-2 (COX-2), which gives rise to elevated concentrations of PGE2 in endometriosis. The cytokine Interleukin-1β (IL-1β), vascular endothelial growth factor (VEGF) and PGE2 itself are also potent inducers of COX-2 in uterine cells. PGE2, in turn, is the most potent known stimulator of StAR and aromatase in endometriotic cells. This establishes a positive feedback loop in favour of continuous oestrogen and PG formation in endometriosis.
Feeding into this loop is arachidonic acid which is synthesised from omega-6 fats commonly found in foods. COX-2 converts arachidonic acid to to PEG2 which directly increases COX-2, creating another feedback loop.
PEG2 increases the rate of the enzyme aromatase, increasing E1, and because the enzyme 17β-HSD is low in edometriotic tissue, this then increases the production of E2.
PGE2 prevents the macrophages of the immune to do a clean up job
Abnormal hormone production by endometriotic lesions is a significant factor that helps endometriotic tissues survive and grow. However alongside this is a critical issue in immune system dysfunction, particularly the reduced ability of immune cells to consume and remove unwanted materials, a process known as phagocytosis. This dysfunction is largely due to macrophages, a type of immune cell responsible for cleaning up debris, not working properly.
In cases of endometriosis, these macrophages are attracted to the peritoneal cavity, an area inside the abdomen, because of inflammation. Ideally, they should remove abnormal endometrial tissue that is present in the peritoneal cavity. However, they often fail to do this effectively in endometriosis, allowing the endometriotic tissue to grow.
The way macrophages function involves two main methods. Firstly, they produce zinc-based enzymes called matrix metalloproteinases (MMPs) to break down the surrounding material of foreign entities. Secondly, they use scavenger receptors (CD36) to enhance the uptake and destruction of cell debris. In endometriosis, however, the function of these macrophages is impaired. In the presence of a high concentration of PGE2, the expression of MMP-9 and CD36 is suppressed. This significantly inhibits the phagocytic ability of macrophages. As a result, the endometrial tissues proliferate in the peritoneal cavity, maintaining and progressing endometriosis.
In essence, the development of endometriosis is not just about the abnormal production of hormones by the lesions but also involves significant dysfunction in the immune system, especially in macrophages. This dysfunction is characterised by a reduced capacity to remove unwanted materials and impaired production of important enzymes and receptors, influenced by PGE2 in the peritoneal fluid.
PGE2 is the likely master of endometriosis
In women with endometriosis, there are two self-reinforcing cycles that keep the levels of PGE2 high in the peritoneal fluid.
PGE2 – COX-2 – PGE2 pathway in macrophages: In peritoneal macrophages (immune cells in the abdominal cavity), PGE2 increases the activity of an enzyme called COX-2, leading to more production of PGE2.
PGE2 – Estrogen – COX-2 – PGE2 pathway in lesions: In ectopic endometriotic lesions (abnormal tissue growths), PGE2 boosts estrogen production, which then increases COX-2 activity, resulting in more PGE2.
High PGE2 Levels then lead to:
Abnormal steroid production: PGE2 leads to unusual production of steroidogenic proteins, like StAR and aromatase. This results in excess production of estradiol, a key hormone for endometrial tissue survival.
Stimulation of growth factors: The estradiol produced by ectopic tissues increases growth factors (like VEGF and FGF), promoting cell growth (proliferation) and new blood vessel formation (angiogenesis).
Direct impact on cell growth: PGE2 directly causes endometriotic and blood vessel cell growth through increased levels of FGF and VEGF.
Reduced macrophage function: PGE2 inhibits the expression of MMP-9 and CD36 in macrophages. This diminishes their ability to clean up debris, aiding the survival and growth of endometriotic lesions.
In essence, elevated PGE2 in the peritoneal fluid maintains a cycle that encourages the development and persistence of endometriosis by influencing increased hormone production and cell proliferation, and immune cell dysfunction.
5. Additional sources of inflammation
Interactions with gut bacteria, blood debris, iron overload, anti-oxidant deficiencies, increased nitrites/nitrates and gene expression of oestrogen metabolism also play a part in maintaining endometriosis.
Bacterial contamination from the gut creates more inflammation and make endometriosis worse via PGE2 Researchers have found that some of the gut microbes linked to bowel problems also feature prominently in endometriosis. When they treated the mice with the broad-spectrum antibiotic metronidazole, the lesions became smaller. Inflammation also was reduced.
Therefore, as well as considering oestrogen/hormone biotransformation in endometriosis, we should also be looking at the gut and vaginal microbiomes for endotoxin-producing bacteria, modulation of the gut ‘oestrobolome’ (bacterial recycling of oestrogen in the gut), endotoxin clearance by the liver and liver support.
Blood debris causes oxidative stress which promotes inflammation It is now widely accepted that oxidative stress, defined as an imbalance between reactive oxygen species (ROS) and antioxidants, may be implicated in the pathophysiology of endometriosis causing a general inflammatory response in the peritoneal cavity. ROS are intermediaries produced by normal oxygen metabolism and are inflammatory mediators known to modulate cell proliferation and to have negative effects.
The body’s complex antioxidant system is influenced by dietary intake of non-enzymatic antioxidants such as manganese, copper, selenium and zinc, beta-carotenes, vitamin C, vitamin E, taurine, hypotaurine, and B vitamins. On the other hand, the body produces several antioxidant enzymes such as catalase, super- oxide dismutase, glutathione reductase, glutathione peroxidase, and molecules like glutathione and NADH. Glutathione is produced by the cell and plays a crucial role in maintaining the normal balance between oxidation and antioxidation. NADH is considered as an antioxidant in biological systems due to its high reactivity with some free radicals, its high intracellular concentrations and the fact that it has the highest reduction power of all biologically active compounds. When the balance between ROS production and antioxidant defence is disrupted, higher levels of ROS are generated and oxidative stress may occur, leading to harmful effects. Oxidative stress is implicated as a major factor involved in the pathophysiology of endometriosis.
Macrophages, red blood cells, and apoptotic endometrial tissue are well known inducers of oxidative stress; therefore, peritoneal production of ROS may be involved in endometriosis. Indeed, activated macrophages play an important role in the degradation of red blood cells that release prooxidant and proinflammatory factors such as heme and iron, implicated in the formation of inflammatory ROS.
Inflammation from excess iron Higher levels of iron, ferritin, and haemoglobin have been found in the peritoneal fluid of affected women than controls. The stroma of endometriotic lesions and peritoneum also revealed the presence of iron conglomerates. Iron overload acts as a catalyst to generate a wide range of ROS, inducing injury to cells.
Treatment with an iron chelator could thus be beneficial in endometriosis, to prevent iron overload in the pelvic cavity, thereby diminishing its deleterious effect.
Inflammation from deficiency of Superoxide Dismutase (SOD): SOD is an important antioxidant system. It catalyses the dismutation of superoxide into hydrogen peroxide and oxygen. SOD shows a decreased activity in the plasma of women with endometriosis, suggesting a decreased antioxidant capacity. SOD requires manganese as a cofactor (see the section on interventions).
Inflammation from deficiency of Glutathione Peroxidase: Glutathione peroxidase is an antioxidant enzyme class with the capacity to scavenge free radicals. This is in turn helps to prevent lipid peroxidation and maintain intracellular homeostasis as well as redox balance. Glutathione peroxidase is localised in the glandular epithelium of normal human endometrium and reaches a maximum level in the late proliferative and early secretory phases of the menstrual cycle.
A study on endometriosis-associated infertility demonstrated a lower mean activity of glutathione peroxidase and increased lipid peroxidation in infertile women with endometriosis compared to women without this disease. This suggests that low level of antioxidant enzymes in the peritoneal fluid plays an integral role in the development of endometrial pathology. Furthermore, in women with endometriosis, abnormal expression of glutathione peroxidase in eutopic and ectopic endometrium has been reported. Overall, this aberrant change in antioxidant enzyme level can be one of the many contributors of the oxidative damage seen in endometriosis (see the section on interventions for approaches to manage glutathione levels).
This suggests that NO plays a role in the pathogenesis of endometriosis, especially in the most aggressive form with intestinal involvement. Additionally, peritoneal macrophages in endometriosis produce more NO in vitro after endotoxin treatment.
Gene Expression of Oxidative Metabolism of Estrogens – methylation, COMT and liver detoxification Increased expression of CYP1A1, CYP3A7, and COMT was observed in endometriosis. Expression of SULT1E1, SULT2B1, UGT2B7, NQO1, and GSTP1 was decreased. These findings exhibit a disturbed balance between phase I and II liver metabolising enzymes in endometriosis, leading to excessive hydroxy-estrogen and altered ROS formation, and stimulation of ectopic endometrium proliferation.
This model suggests increased 2-hydroxylation and 16α-hydroxylation and high 4 hydroxylation of estrogens together with high methylation, lower sulfatation and glucuronidation of CEs and 16α-OH-estrogens in endometriosis. This imbalance between phase I and II metabolic enzymes can result in excessive 2- and 16α-OH-estrogen and corresponding oestrogen quinone formation. The first could be involved in maintaining strong oestrogen agonistic activity in endometriotic tissue, while the second might be a source of excessive ROS generation. Moreover, altered NQO1 isoform distribution could result in impaired detoxification of toxic quinone oestrogens and may contribute to over enhanced ROS production in endometriosis. Apart from E2, 4-OH-, 16α-OH-estrogens and ROS can also be responsible for excessive growth of ectopic endometrium in ovarian endometriosis. ROS scavengers, or even antioxidant nutrients, might, therefore, influence the proliferation of ovarian endometriotic cells.
6. Disrupting the feedback loops, reducing PEG2 and supportive anti-oxidants are effective treatments for endometriosis
Understanding the biochemical pathways involved in the maintenance and progression pf endometriosis provides targets for interventions to reduce and manage inflammation and lesion growth.
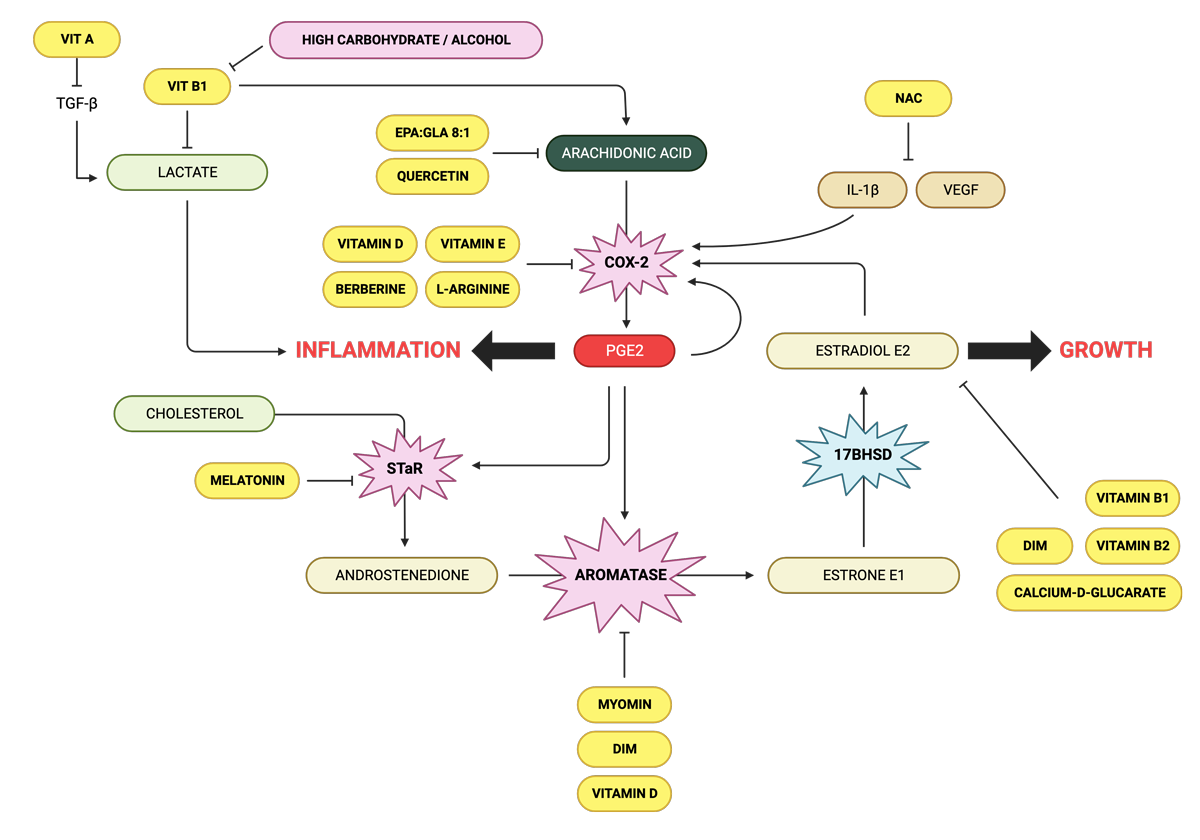
Arachidonic acid inhibitors
EPA:GLA ratio of 8:1 Essential fatty acids (EFAs) are biologically active fats which the body requires to support several important functions from blood clotting to inflammation; differentiating them from other fats which are either stored or used for energy. EFAs are deemed ‘essential’ because humans and other animals cannot produce them; meaning that they must be consumed from food.
The two types of fatty acids which are essential to the body are omega-3 (ALA) and omega-6 (LA). Other fatty acids such as EPA, DHA and GLA are considered ‘conditionally essential’ as they may become essential under certain developmental or disease conditions.
Arachidonic acid, derived from LA is found in meat, eggs and dairy, and is needed to support muscle growth, brain development and a healthy nervous system. However, we only require very small amounts of this fatty acid and when consumed in excess, it can promote inflammation.
Quercetin Quercetin is found many fruits and vegetables including citrus fruits, apples, onions and strawberries, and is known to reduce inflammation. It does this by interfering with the production of arachidonic acid. Specifically, quercetin stops the creation of inflammatory mediators like PGE2 and leukotrienes. These mediators are not only involved in causing inflammation but also play a role in controlling how the uterus contracts. Quercetin has been shown to significantly reduce endometrial lesions.
Lactoferrin is an iron metabolism regulator. Heavy bleeding leads to iron loss and anaemia, but taking iron can feed bacteria and cause more pain and inflammation. Lactoferrin can regulate iron metabolism without these concerns.
Reducing systemic oestradiol (from the ovaries, gut and adrenals)
Vitamins B1 and B2 maintain oestrogen detoxification by the liver, and a deficiency can lead to excess estradiol. Alcohol and high carbohydrate diets increase the need for vitamin B1 and supplementation would be required.
Calcium D-glucarate is a natural compound found in fruits and vegetables. It works by inhibiting the activity of beta-glucuronidase made by gut bacteria, an enzyme that helps to circulate oestrogen back into the body from the gut.
There is a very strong association with many autoimmune diseases and endometriosis, Hashimoto’s thyroiditis probably being the most prevalent, as well as lupus, antiphospholipid syndrome, scleroderma and multiple sclerosis. 3 common gene fingerprints – known as haplotypes – are prevalent with women with endometriosis. One of these haplotypes accounts for about 90 percent of all autoimmune disease an includes celiac disease, which is why cutting out gluten can have a tremendous benefit symptomatically (see the section on interventions for dietary recommendations).
Endometriosis is often associated with Restless Leg Syndrome (RLS) an irresistible urge to move the legs due to an unpleasant non-painful sensory disturbance, described in a variety of ways for example as crawling, creeping and pulling. RLS is associated with dopamine deficiency. Dopamine is a neurotransmitter which mediates multiple functions in the body and its deficiency is associated with
low moods
depression
fatigue
lack of motivation
inability to experience pleasure
insomnia
trouble getting going in the morning
mood swings
forgetfulness
memory loss
inability to focus and concentrate
inability to connect with others
low libido
sugar cravings
caffeine cravings
inability to handle stress
inability to lose weight
Research shows that women with moderate to severe endometriosis have a higher than normal frequency of genes which show mutations – polymorphisms – in dopamine receptors – dopamine receptor D2 (DRD2). The presence of polymorphism 2 could cause a defect in a post-receptor signalling mechanism, resulting in a mild increase in serum prolactin levels. Prolactin has angiogenic activity which may promote implantation of ectopic endometriosis tissue.
The use of high doses of dopamine agonists may cause an increase in the number of receptors that can make the post-receptor signalling mechanism work properly with this compensation, despite the presence of the polymorphism.
9. My approach to Managing Endometriosis – A pain-free Life is Possible
The biggest breakthroughs in the management of endometriosis has come studies showing that nutrition, detoxification and supplements can effectively and significantly reduce pain and inflammation.
Nutrition
While there is no one-size-fits-all diet for endometriosis, there are certain foods that can exacerbate inflammation and make symptoms worse, and others that can help reduce inflammation and promote healing.
As an oestrogen-driven condition, nutrition has to focus on preventing excess oestrogen and other hormone intake. For this reason I recommend:
avoiding red meat and focusing on seafood for protein. Protein is important for tissue repair and hormone balance, but it’s important to choose lean sources to avoid excess saturated fat. Omega-3 fatty acids, found in fatty fish like salmon and sardines can help reduce inflammation and promote hormonal balance. A diet high in fish and seafood is ideal for endometriosis.
avoiding cow’s dairy
avoiding soya
avoiding high sugar foods. High sugar drives insulin which can increase oestrogen.
For lowering inflammation I recommend:
avoiding gluten and all grains
avoiding all processed foods. These are often high in sugar, salt, and unhealthy fats, which can exacerbate inflammation and worsen symptoms.
avoiding artificial sweeteners, which disturb the gut microbiome.
avoiding pro-inflammatory seed oils like sunflower oil and focusing on monounsaturated fats, found in foods like avocado and olive oil.
avoiding coffee. Caffeine can worsen symptoms, so it may be worth experimenting with avoiding or reducing this to see if it helps.
include vegetables with every meal. These are rich in fibre, vitamins, minerals, and antioxidants, which can help reduce inflammation and promote healing. Choose a variety of colourful fruits and vegetables, including leafy greens, berries, citrus fruits, and cruciferous vegetables like broccoli, cauliflower, and Brussels sprouts.
Include plants that help to detoxify oestrogen via the liver:
Artichoke hearts
Bok choy
Broccoli
Brussels sprouts
Cabbage
Cauliflower
Greens: beet greens, kale, chard, collard, mustard greens and rocket
Onions, garlic, and scallions
Oregano
Rosemary
Sage
Thyme
Gut and Vaginal Microbiome Restoration, and Detoxification
Healing intestinal and vaginal microbiome imbalance and supporting liver detoxification restores hormone balance and remove sources of inflammation.
Supplements
The nutrients discussed above support hormone metabolism and reduce inflammation, but I just want to note that 4 supplements have made the most difference in my clinical experience: vitamin E, vitamin D, NAC and methylated B complex in high doses.
17 Beta Estradiol on day 21 of the cycle from 184pg/ml to 171 pg/ml.
Lifestyle
For detailed lifestyle approaches (and additional discussion) please enrol on my free course, Endometriosis Explained
10. Takeaways
Endometriosis is a complex condition that involves immune dysregulation, inflammation and a dominance of circulating oestrogen.
Endometriosis most likely starts with differentiation and migration of any Mullerian tissue during the formation of the embryo resulting in patches of this tissue being laid down in abnormal locations in the pelvis or elsewhere in the body. Later in life, these misplaced patches of tissue develop into endometriosis when they are exposed to oestrogen.
Silent endometriosis may be a cause of infertility
The maintenance of endometriosis is largely mediated by prostaglandin E2 which leads to increased growth of lesions and inflammation
High levels of prolactin mediate pain and can be reduced with dopamine boosters
Increased risk with chemicals commonly found in plastic and cosmetics.
Increased risk with imbalanced gut and vaginal microbiomes
Increased risk with genetic variants of COMT and MTFHR genes
A hormone balancing diet is essential
Multiple supplements are supportive in prevention and treatment particularly vitamin E, NAC, vitamin D and methylated B vitamins
The controlling factor in fibroids is excess oestrogen producing oxidative stress (inflammation) causing DNA damage which goes on to cause symptoms. The shrinking of fibroids depends on reducing oestrogen levels, repairing DNA damage with vitamin D and managing inflammation with antioxidants.
Fibroids are the most common growths in the uterus. Their growth is stimulated by oestrogen and progesterone, causing uterine collagen to cross-link and harden, creating a stiff mass of collagen fibres. Fibroids tend to develop in early perimenopause, when oestrogen levels increase and regress in menopause as oestrogen declines. Fibroids tend to have more oestrogen receptors, so this may be one reason oestrogen disproportionately affects the growth of these solid tumours. More than 80% of Black women and nearly 70% of white women have fibroids by age 50. Sometimes these growths are harmless and can even go undetected, but in many cases they cause symptoms ranging from pain and bleeding to infertility.
1. Early warning signs
The symptoms of fibroids are relatively common and can be associated with other factors or diseases, such as ovulatory dysfunction, endometriosis or endometrial polyps. Many women do not connect their symptoms to fibroids, so can go undiagnosed for some time, and some fibroids can be asymptomatic, thereby avoiding detection. Many women have uterine fibroids and don’t even know it. Small fibroids don’t often cause symptoms and don’t regularly affect your life. However, larger fibroids may lead to several warning signs, including:
Heavy bleeding: you can experience heavy menstrual bleeding, large clots, and bleeding between cycles when you have one or more uterine fibroids. This is the most common symptom. Excessive bleeding can lead to the development of anaemia (low red blood cells) causing ongoing tiredness and weakness.
Pelvic pressure or pain, lower back pain: pelvic pain and low back pain are common early symptoms of uterine fibroids. The pain may be sharp or feel similar to your menstrual cramps but worse.
Full feeling in the abdomen: as uterine fibroids grow, they occupy more space in your uterus and pelvic area. You may feel like your belly is full, as if you’ve eaten a large meal.
Increased urination: you might feel like you have to urinate more often when you have uterine fibroids. This happens when the fibroid is big enough to put pressure on your bladder. Although rare, fibroids can also cause obstruction of the ureter, which might require treatment if this progresses to severe hydronephrosis.
Pain during sex: the fullness in your abdomen that fibroids cause can also lead to discomfort during sex. Not everyone feels this, but if you have pain with intercourse, getting evaluated for uterine fibroids is a good idea.
Gastrointestinal symptoms: constipation or the recurrent need to void bowels can also be caused by fibroids.
Rarely, a fibroid can cause sudden, serious pain when it outgrows its blood supply and starts to die. Get medical care right away if you have severe bleeding from the vagina or sharp pelvic pain that comes on fast.
There are long-term complications that can affect the integrity of the endometrium, the uterine lining. This means it can be difficult getting pregnant. During pregnancy, women with fibroids have an increased risk of complications compared with women without fibroids, including
preterm delivery (16.7% versus 6.3%) and
premature rupture of membranes (14.3% versus 2.1%)
risk of placental abruption (7.5% versus 0.9%)
fetal malformation (6.2% versus 3.3%)
caesarean section (70–76% versus 32.8%)
postpartum haemorrhage (33% versus 6%) and
foetal malpresentation (19% versus 4.4%) are increased in women with fibroids
Fibroids can also be associated with miscarriage.
The symptoms of fibroids are relatively common and can be associated with other factors or diseases, such as ovulatory dysfunction, endometriosis or endometrial polyps. Many women do not connect their symptoms to fibroids, so can go undiagnosed for some time, and some fibroids can be asymptomatic. Lack of symptoms does not necessarily mean lack of inflammation, so women experiencing infertility should be evaluated to the presence of fibroids.
2. Presentation and Diagnosis
Diagnosing fibroids is usually done by transvaginal ultrasound, although this is limiting if the uterus extends beyond the pelvis, a common problem with this disease. Abdominal ultra-sonography might be required to diagnose fibroids that extend beyond the effective range of the trans-vaginal probe, but then MRI is generally preferred.
Women often have more than one fibroid. They can be different in size and in their location. The location of fibroids directly affects the symptoms they induce, as well as the time to the manifestation of such symptoms. For example, submucosal fibroids that bulge into the uterine cavity seem to have more of an effect on abnormal menstrual bleeding and pregnancy problems. This is independent of fibroid size as small fibroids that protrude into the uterine cavity can also induce menstrual irregularities. Conversely, subserosal fibroids that form on the outside of the uterus are slow growing and considerable time is needed before they are of a sufficient bulk to cause symptoms, such as back, leg or pelvic pressure and abdominal and pelvic pain.
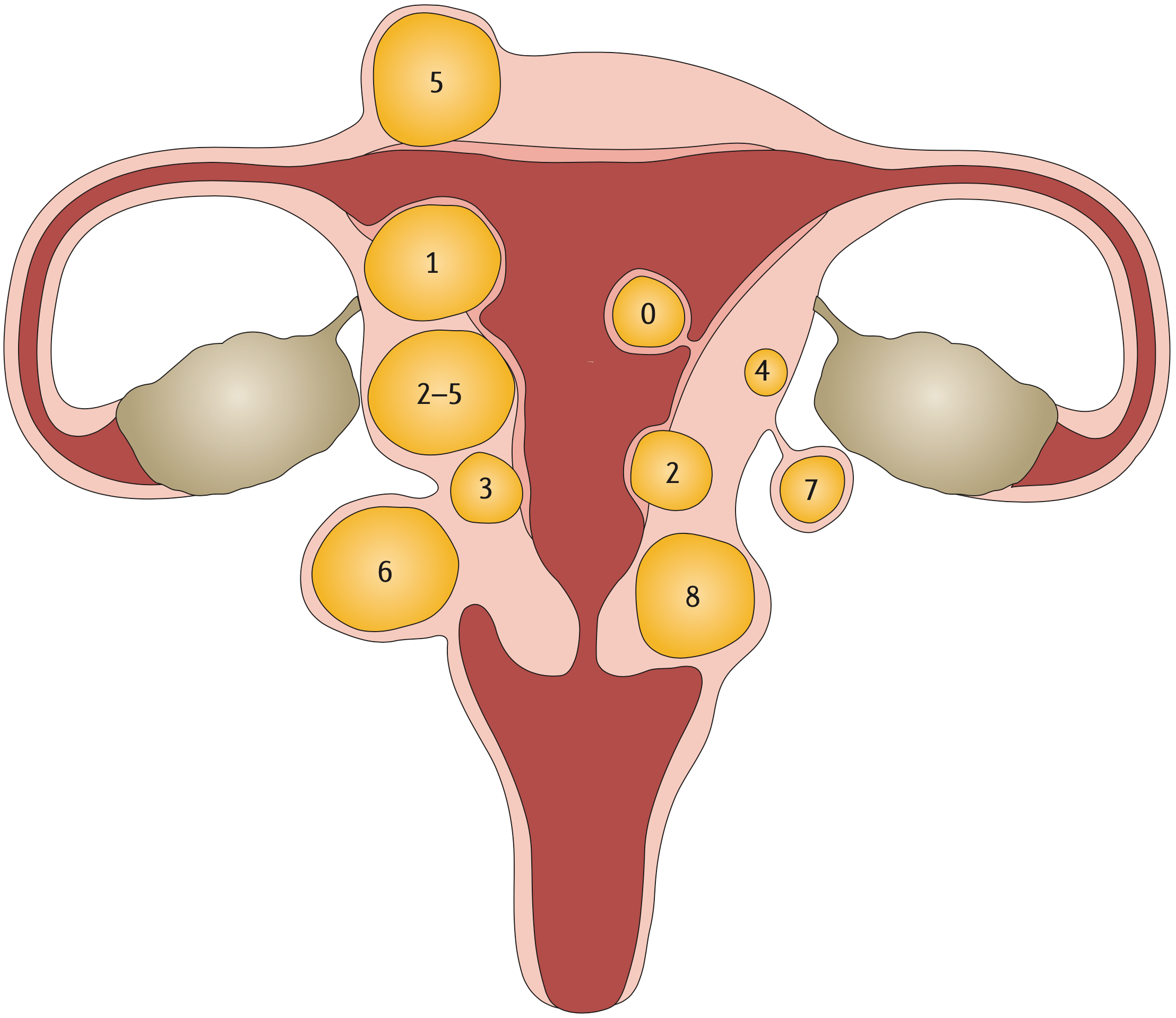
The International Federation of Gynecology and Obstetrics (FIGO) has established a classification system which uses an 8-point numerical system to describe the location of fibroids relative to the endometrium (submucosal surface) and the serosal surface, with low numbers indicating a central location.
Type 0: pedunculated fibroid, which is localized in the submucosa and extends inside the uterine cavity
Type 1: submucosal fibroid, with <50% in an intramural location
Type 2: submucosal fibroid, with ≥50% in an intramural location
Type 3: contacts the endometrium, with 100% in an intramural location
Type 4: intramural fibroid
Type 5: subserosal fibroid, with ≥50% in an intramural location •
Type 6: subserosal fibroid, with <50% in an intramural location •
Type 7: subserosal pedunculated fibroid
Type 8: other (for example, cervical or parasitic)
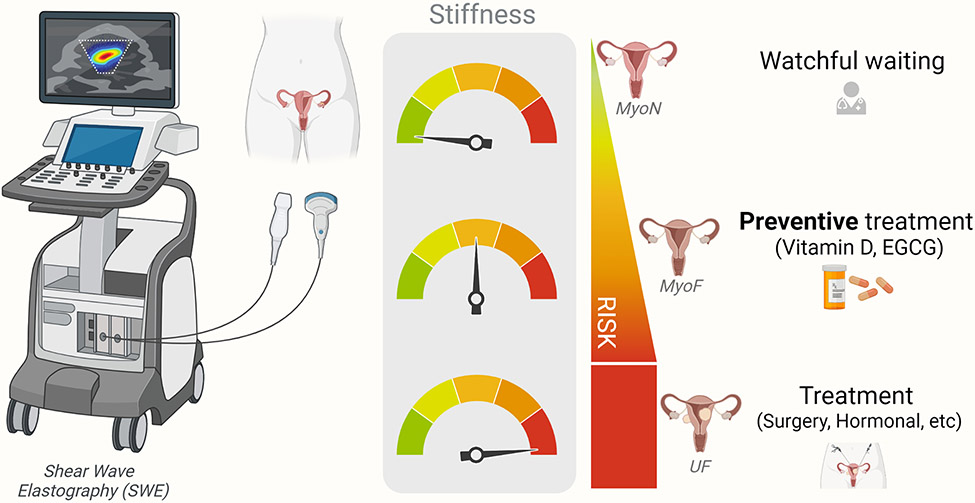
Proposed application of SWE as a screening tool for identification of women at risk of fibroid development and corresponding preventive measures to be taken. MyoN: normal non-fibroid myometrium; MyoF: at risk-myometrium, EGCG: Epigallocatechin Gallate.
The principle of SWE is to use sound waves to produce images. The sound waves can give an indication of how stiff the uterine tissue is: soft, firm, solid or hard. The stiffness indicates the progression of fibroid growth, as well as the use of appropriate therapies.
3. Biomarkers
In urine
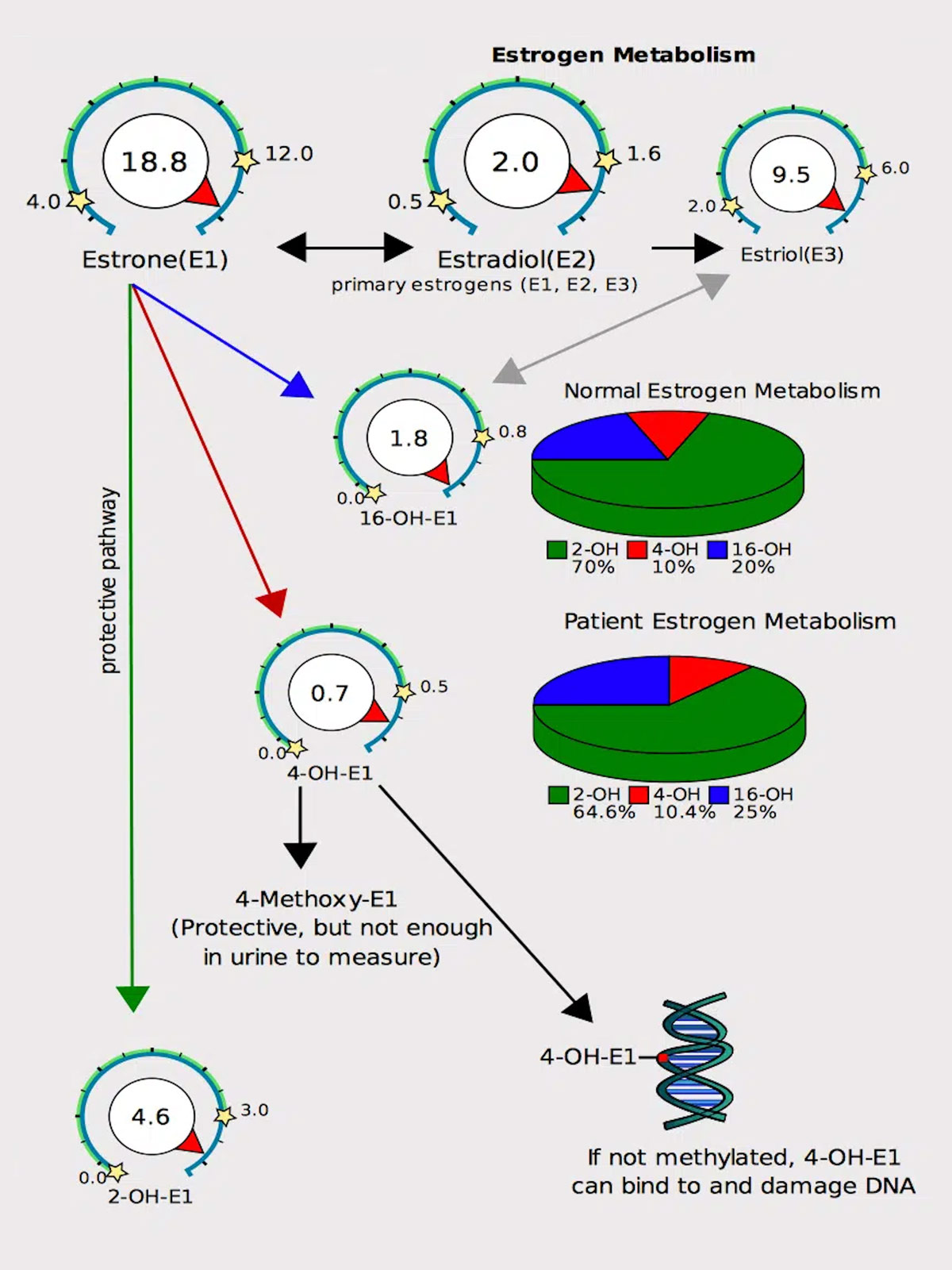
As oestrogen can fuel the growth of fibroids, it can be helpful to identify whether oestrogen is elevated, and how it’s metabolised. DUTCH urine testing is unique because it helps identify symptoms of hormonal imbalances by providing a complete picture of hormone levels which cannot be seen in testing serum (blood) alone. The DUTCH test can measure the levels of the 3 types of oestrogen, oestrone (E1), oestradiol (E2) and oestriol (E3) and how they are metabolised.
Estradiol (E2) is the most biologically active estrogen in the body. However, estrone (E1) and the phase 1 estrogen metabolites (2-OH, 4-OH, 16-OH) can also bind to estrogen receptors. Thus, it is possible that elevations in any of these markers may contribute to fibroid growth.
The phase 1 metabolite, 16-OHE1, tends to bind more tightly to oestrogen receptors than the 2-OH and 4-OH metabolites (but not nearly as tightly as E2), and is known to cause tissue groeth. If too much oestrogen is metabolised into the 16-OHE1 form, it may contribute to increased fibroid growth.
Having this information is extremely valuable, because it means that as a practitioner I can first reduce the amount of oestrogen and alter the metabolism of oestrogen in a more favourable way.
In blood
The CA-125 blood test measures the amount of CA125 protein that both women and men have in their blood. CA-125 is elevated in cases of fibroids, endometriosis and adenomyosis, as well as ovarian cancer. This means that it can’t be used to identify any one of these conditions, but it can be used to monitor progression.
4. Development and Progression of Fibroids
Fibroids are associated with high oestrogen levels, or oestrogen dominance. Obesity and the perimenopausal state are often associated with higher oestrogen levels. Studies have shown that oestrogen levels are actually higher in perimenopausal women, and fat is hormonal organ capable of producing oestrone, a strong oestrogen. The inflammatory mediators interleukin-2 (IL-2), IL-6, tumor necrosis factor-alpha (TNF-alpha), and leuko- triene B4 (LTB4) are also produced in the adipocyte and contribute to fibroid formation.
MED12 gene mutations created by high oxidative stress in the uterus drive fibroid formation
Nearly 70 percent of uterine fibroids are linked to a mutation in the MED12 gene but recreating this problem in the lab has proven to be difficult because when cultured, the mutant cells in the fibroids do not survive. This year scientists used CRISPR-based genome editing technology (for which 2 women scientists won a Nobel prize in 2020) to precisely engineer cells that have the same mutation in the MED12 gene. After successfully culturing the mutated fibroid cells in 3D spheres, it was found that the cells produced heightened levels of collagen, a key feature of uterine fibroids, as well as other chromosomal abnormalities commonly seen in uterine fibroids.
A clear connection has been made between MED12 mutations and high levels of oxidative stress in the uterus. The direct connection between oxidative stress and MED12 is not yet clear however almost all the risk factors below can drive oxidative stress.
What is oxidative stress?
Biochemical reactions in the body leave toxic residues – (commonly known as reactive oxygen species or free radicals) – that can damage cellular components such as DNA, proteins, and lipids. Antioxidants can neutralise free radicals and repair damage. In a healthy state, the body maintains a balance between the generation of free radicals and the antioxidant defences that neutralise them.
When the generation of reactive oxygen species overwhelms the body’s antioxidant defences, oxidative stress occurs. This imbalance can result in cellular and tissue damage,
Several factors, including environmental pollutants, smoking, poor diet, and physical stress, can lead to an overproduction of these reactive oxygen species.
5. Risk Factors
Anything that increases oestrogen:
Age Increasing age is a significant risk factor for uterine fibroids, especially among women at the premenopausal stage and those ≥ 40 years of age. For instance, 60% of African American women aged 35-49 years reported uterine fibroids, whereas 80% of those aged ≥ 50 have uterine fibroids. Among White women, 40% of those aged ≤ 35 years and 70% aged ≥ 50 years developed uterine fibroids. Rapid growth of fibroids after the age of 30, especially in perimenoause, is consistent with age-related changes in oestrogen and progesterone. Fibroids have not been detected in prepubertal girls, and only sporadic cases have been reported in adolescents. However, the factor(s) involved in their development at such an early age is unknown. Due to the slight difference in biochemical pathways, uterine fibroids in young women do not exhibit typical uterine fibroid biology. In several cases, adolescent patients had a translocation between chromosomes 12 and 14, which is a confirmed risk factor for uterine fibroids. Women at the menopausal stage have shrunk uterine fibroid lesions and decreased sex hormones.
Early first period Women with an earlier age at menarche had higher levels of estradiol and estrone and lower levels of sex hormone-binding globulin than women with a later age at menarche.
Red meat? A diet higher in protein is protective however there has been a question mark around the risk of red meat increasing oestrogen. A study measuring the concentrations of oestrogen in American and Japanese beef found that the median concentrations of E2 and E1 in USA beef fat were 140 times and 11 times, respectively, higher than those in Japanese beef fat. In red meat, E2 and E1 levels of USA beef were ∼600 times and 10 times, respectively, higher than those of Japanese beef. It’s likely that the very high levels of E2 and E1 in American beef derive from the steroids given to the cattle. On the other hand, nearly zero level of E2 seen in Japanese beef was considered to be the natural endogenous status in beef without steroids. The go on to say “Accordingly, it is our intuitive feeling that the increasing consumption of oestrogen-rich beef following steroid implantation might facilitate oestrogen accumulation in the human body and could be related to the incidence of hormone-dependent cancers”, and very likely fibroids.
HRT A state-of-the-art literature review found that some combinations of oestrogen and progestin have exhibited a significant influence on fibroids enlargement, as well as in frequency of newly detected fibroids in menopause. By contrast, several studies failed to demonstrate a significant increase in fibroids size, although a trend towards enlargement was noted. Women should have regular thorough follow-up, including trans-vaginal ultrasound for the monitoring of fibroid size, and HRT should be discontinued if an increase in size of uterine fibroids is documented.
Obesity Fat tissue, has been proven to play hormonal, metabolic, and immune regulatory roles in the body. Fat cells make leptin, a hormone which in excess can promote inflammation driving fibroid growth. Additionally fat cells create a fibroid-friendly micro-environment that can induce fibrosis and fuel fibroid growth by increasing blood supply to it. Each kilogram of excessive body weight is correlated with an increased risk of uterine fibroids development. A study conducted in the United States found that women diagnosed with uterine fibroids are heavier than those without uterine fibroids. Moreover, an increase in the body mass index (BMI) by one unit, higher waist-to-hip ratios, and body fat percentage exceeding 30% increase the risk for uterine fibroids. Abdominal visceral fat also enhances this risk. Obesity and particularly excess visceral fat may be complemented with the reduced production of the sex hormone-binding globulin (SHBG), which binds circulating hormones, disrupting the hormonal activity toward sensitive tissues, and thereby influencing the delicate hormonal balance in the body.
Alcohol Alcohol and especially beer are known to increase oestrogen. A recent Korean study assessed alcohol consumption and the risk of new-onset fibroids in 2.5 million Korean women aged 20 to 39 years concluded:
Mild-to-Moderate Drinkers vs. Heavy Drinkers: Women who consumed alcohol had a higher chance of developing uterine leiomyomas. The increase in risk was between 12% and 16%. Specifically, women who drank alcohol mildly to moderately had about a 12% higher risk, while heavy drinkers had about a 16% higher risk.
Frequency of Drinking: The risk of developing these tumors increased with the frequency of alcohol consumption. Women who drank once a week had an 11% increased risk, while those who drank three or more times a week had a 15% increased risk.
Amount of Alcohol per Session: The risk also increased with the amount of alcohol consumed per session. Drinking seven or more glasses of alcohol in one session was associated with a 17% increased risk.
Sustained Drinkers vs. Sustained Non-Drinkers: Women who consistently consumed alcohol over a period of time (referred to as “sustained drinkers”) had a 20% increased risk of developing these tumors compared to women who consistently did not drink alcohol (referred to as “sustained nondrinkers”).
Change in Drinking Habits: Women who stopped drinking alcohol showed a small increase in risk (3%), whereas women who started drinking who previously did not have a 14% increased risk.
In summary, the study found that drinking alcohol is associated with a higher risk of developing uterine leiomyomas, and this risk increases with the amount and frequency of alcohol consumption. Women who consistently drink have a notably higher risk compared to those who don’t drink or those who stopped drinking.
An imbalanced gut microbiome The estrobolome is a collection of bacteria in the gut which is capable of metabolising and modulating the body’s circulating oestrogen. The gut bacteria regulate oestrogens through secretion of β-glucuronidase, an enzyme that splits detoxified oestrogen, releasing free oestrogens that are then reabsorbed into the bloodstream and repeatedly circulated through the body, increasing oestrogen levels. The genes for β-glucuronidase are widely found in Firmicutes (which are increased in the vaginal microbiome in women with fibroids, see below).
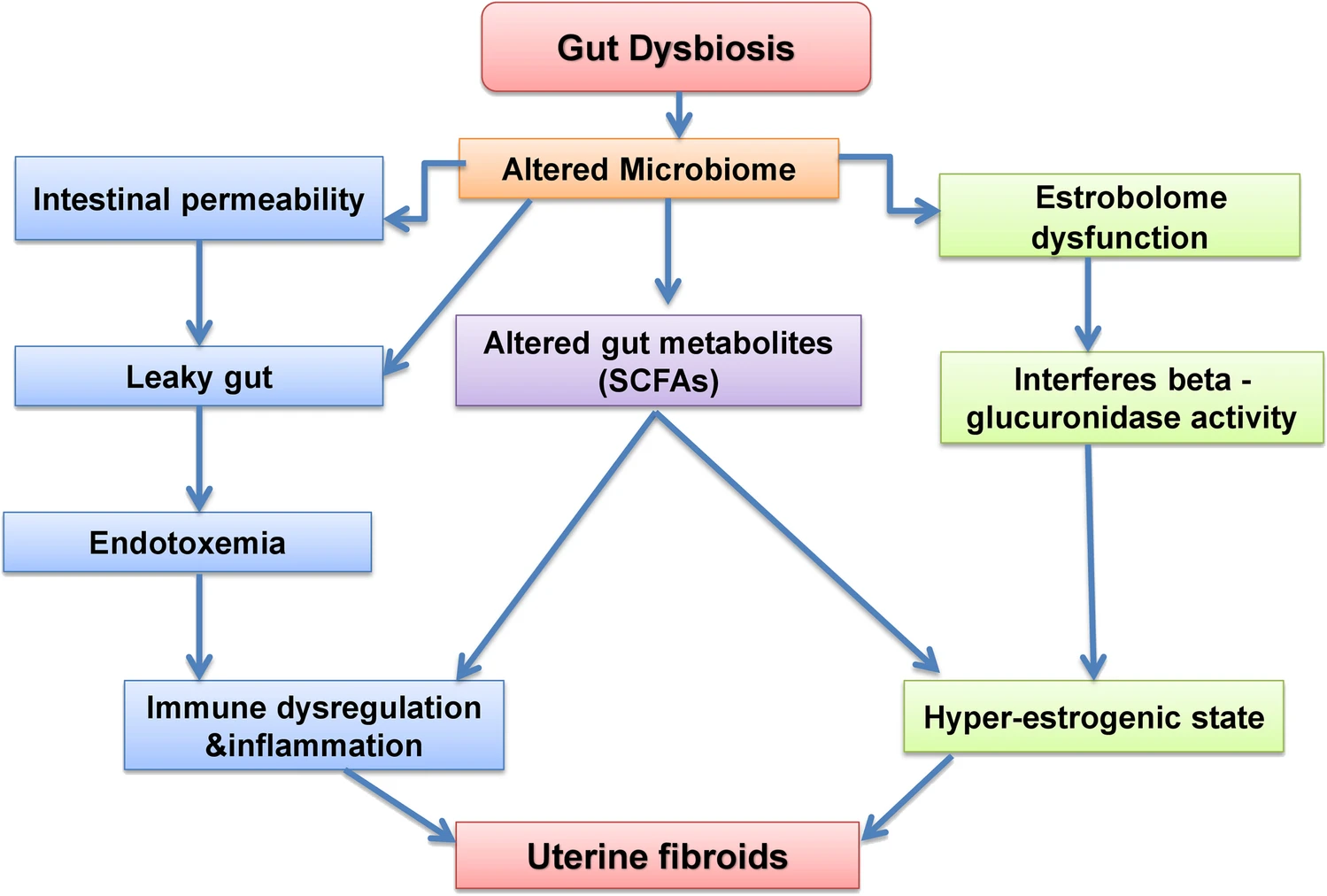
A dysbiotic gut results in an altered microbiome which triggers the following pathways
interferes with the estrobolome functioning and results in hyperestrogenic state leading to uterine fibroids
altered levels of gut metabolites such as short chain fatty acids (SCFA) which triggers immune dysregulation and induce inflammation and also leads to hyperestrogenic state
interferes the gut permeability leading to a leaky gut and toxicity which could dysregulate the immune function.
COMT Catechol-O-methyltransferase (COMT) is an enzyme that triggers enhanced transformation of 2-hydroxyestradiol (anti-estrogen) into 2-methoxyestradiol (pro-estrogen) with resultant hyperestrogenic environment that may contribute to cell proliferation and increase in fibroid development. High COMT activity has been found in fibroids. Women with the high-activity COMT Val/Val genotype are 2.5 times more likely to develop fibroids than women with other genotypes. The prevalence of this genotype was significantly higher in African American women (47%) compared with white (19%) or Hispanic (30%) women.
MTFHR Methylenetetrahydrofolate reductase (MTHFR) plays a key role in the enzymatic process in the folate metabolism pathway, which converts folic acid (obtained from food and/or supplements) into methyl-folate (the form of folate used by your body), and then participates in DNA synthesis, modification and methylation. The mutation of the MTHFR C677T gene leads to the disorder of folate metabolism, the decrease of antioxidant capacity, the increase of uterine related oxidative stress, and the proliferation of uterine smooth muscle cells, thus leading to the formation of fibroids. Additionally MTHFR mutations can cause high blood pressure via increased homocysteine. Vitamin B2 (riboflavin) is a required cofactor for MTFHR and higher vitamin B2 levels are associated with increased MTHFR enzyme activity, lower homocysteine and improved blood pressure.
Genetic testing has identified:
The wildtype (non-variant) MTHFR 677 shown as “CC”. This is associated with 100% enzyme activity and does not increase risk for higher homocysteine or high blood pressure.
A single MTHFR 677 variation shown as “CT”. This results in 30-35% reduction in enzyme activity and can slightly increase risk for higher homocysteine levels and blood pressure.
A double MTHFR 677 variation shown as “TT”. This results in 60-70% reduction in enzyme activity and increases the risk for higher homocysteine and high blood pressure.
A study this year reported that women with untreated hypertension faced an 18% higher risk of developing uterine fibroids when compared to those without hypertension. Conversely, women with hypertension who were using blood pressure medications had a 37% lower risk of developing uterine fibroids, with the use of angiotensin-converting enzyme inhibitors associated with a 48% lower risk. Interestingly, women with new-onset hypertension had a 45% greater risk of uterine fibroid diagnosis, while those with pre-existing hypertension had little additional risk. The formation of fibroids is attributed to the chronic destruction of the uterine lining due to increased blood flow and inflammation.
Vitamin D deficiency
A systematic review last year concluded that 100% of all research studies identified vitamin D deficiency in women with uterine fibroids. The best estimate of the effect of hypovitaminosis D on fibroid development found that deficient vitamin D (< 20 ng/mL) increased the risk of uterine fibroids by 32%. The importance of this relationship is underscored by the prevalence of vitamin D deficiency, a condition which affects approximately 80% of Black American women, a population disproportionately affected by fibroids.
Women at risk for deficiency should be screened and those with deficiency should take supplements. The functional range for vitamin D is 125-150. I usually recommend 10,000 IU a day at deficiency below 60 and test serum levels regularly to avoid any overdose-related toxicities. Routine vitamin D supplementation for women with insufficiency may provide effective treatment and prevention of fibroids.
Imbalanced vaginal microbiome
A recent study showed that an increased level of the bacterial phyla Firmicutes was observed in both the cervical and vaginal microbiome of women with fibroids. An increased level of Firmicutes is associated with obesity. Firmicutes include Lactobacillus, Streptococcus, Clostridia, and can be reduced with high animal protein diet.
Uterine infections
Fibroids are associated with Chlamydial infection, and pelvic inflammatory disease. The risk of fibroids is increased 5x when infections are associated with the copper coil.
Copper Intrauterine Devices (IUD)
The copper coil may be a cause of uterine fibroids. Intrauterine devices can cause local irritation, pressure, inflammation, and tissue changes in the uterus. Copper IUDs in particular impact cellular mechanisms in the endometrium. There may be oedema, vascular congestion, cell death, and other cytological alterations. These effects involve inflammatory cytokines and changes in cell proliferation and activity that have been associated with fibroids: Interleukin 1 beta (IL-1β) and tumour necrosis factor-alpha (TNF-α) levels were high in the late secretory phase and IL-6 levels were high in the proliferative early secretory phase in IUD-subjected endometrial samples. The expression of IL-1, IL-6, and TNF-α was found to be associated with the pathophysiology of uterine fibroids. A study concluded that the use of copper IUDs for more than 2 consecutive years should be avoided in order to prevent oxidative damage.
Copper T380A is one of the most commonly prescribed IUDs and has been shown to significantly increase copper levels. The use of copper T-200 IUD for 12 months significantly increased copper levels and significantly decreased zinc and iron levels. It is suggested that the low zinc status was probably responsible for the heavy bleeding which was common among the study group using copper IUDs, which in turn was responsible for the anaemia seen in more than 50% of the IUD users.
The adverse effects of copper intrauterine devices (IUDs) such as abnormal bleeding, pain and cramps may be due in part to the burst release of copper ions during the first few months of usage. Copper can then continue to build up slowly in the body. Coppertoxic.com reports: “For many women, symptoms often first begin appearing 2 or 6 months after insertion. For others, the time period may be much longer, years to decades, before they notice anything, or connect the dots. Side effects of the copper IUD as copper accumulates usually begin with increasing brain fog and fatigue, often paired with a racing mind. Eventually, once the liver is overloaded, copper will then start accumulating more in the brain, and severe shifts in personality can occur as a result of increasing bio-unavailable copper and calcium and changes in neurotransmitter production. The period 2 to 5 months post-insertion is a common time for many women when metabolism begins slowing and energy, behaviour, and reactions begin changing, especially with a tendency towards increasing depression and irritability.”
Estrogen is known to increase copper absorption vice versa. Having an excess of copper in the body has been linked to being one of the key underlying drivers of anxiety, oestrogen dominance, painful periods, heavy periods, irregular periods, mental health issues, and overall hormonal imbalances.
Toxic pollutants
Common chemicals called phthalates found in hundreds of household products have been linked to fibroids. Phthalates are present in many household items ranging from food packaging and processing equipment to shower curtains, building materials, and car interiors. Phthalates are also used as solvents in cosmetics and other personal care products and to coat or encapsulate certain pharmaceutical pills and dietary supplements. The chemicals can leach out of these products and enter food, air, and water, meaning you can swallow, inhale, or absorb these phthalate particles through direct skin contact. The body then metabolises these chemicals, yielding byproducts that several studies have detected in human urine, breastmilk, and blood.
A systematic review and application of social, structural, and political context to racial disparities in uterine fibroids found that Black women face worse clinical and surgical outcomes than their white counterparts. The differences in gene expression in fibroids from Black and white women, as well as racial disparities in fibroid prevalence, they say, may reflect that Black individuals disproportionately experience exposures linked with increased risk for uterine fibroids.
This includes a higher risk of chronic psychological stress, adverse childhood experiences, perceived racism and environmental contaminant exposures like air pollution among Black women, which have all been associated with a higher risk for developing and experiencing severe symptoms from fibroids.
Racial disparities may also stem from other social determinants of health such as a higher fat diet, lower levels of physical activity, vitamin D deficiency, as well as individual behaviours such as use of chemical hair relaxers that contain chemicals that are associated with increased risk of uterine fibroids. Studies have also suggested racial disparities in uterine fibroids and endometriosis can be linked to a lack of adequate access to health care, authors note, including minimally invasive gynecologic surgeons, interventional radiologists, and bias and discrimination within the health care system. “Black women may be more likely to have symptoms dismissed, report negative experiences with the health care system and wait too long to see a specialist, which delays diagnosis and treatment,” the author said. “These significant differences in experiences, access and dismissal or misattribution of symptoms may lead to worse outcomes.”
While some women with fibroids don’t have symptoms, others have significant pain, anaemia, heavy menstrual bleeding, increased urinary frequency, fertility problems and pregnancy complications. Black women are diagnosed with fibroids roughly three times as frequently as white women, develop them earlier in life and tend to experience larger and more numerous fibroids that cause more severe symptoms. The author of the study said “If we are sincere about striving for health equity, then we have to look at the underpinnings of inequity in our healthcare system and in society. Solutions need to address root causes of disparities through policy, education and programs that ensure all patients receive competent care.”
6. Associations
Association with Breast Lumps (fibroadenoma)
The same mutated MED12 gene that is found to cause fibroids is also found in 59% of breast fibroadenomas. This indicates that benign tumours of the breast and uterus, both of which are key target tissues of oestrogen, may share a common genetic basis underpinned by highly frequent and specific MED12 mutations. Interestingly supplementing with iodine resolves breast lumps and breast pain which may indicate that iodine deficiency is also a driver for fibroid development.
Tissues that store iodine include the thyroid, breasts, ovaries, uterus and placenta. While the thyroid tends to concentrate a higher percentage of iodide (I¯), other tissues tend to utilise a greater percentage of molecular iodine (I₂), which exerts multiple and complex actions related to its role as an antioxidant, an anti-inflammatory, a pro-inflammatory, an inducer of cell death, an immune modulator, and a promotor of cell differentiation. Importantly, iodine helps to maintain the oestrogen balance in favour of estriol which has been shown to protect against oestrogenic cancers and decrease the risk of fibrocystic changes in the breasts.
High oestrogen levels can prevent the absorption of iodine, which may be an additional cause of fibroid development. Iodine deficiency has been associated with fibrocystic breast disease and, more recently, with the development of distant metastatic breast cancer in young women aged 25-39. This trend toward the development of breast cancer in younger women has been associated with the reemergence of iodine deficiency in the U.S. since the 1970s. Since iodine protects against abnormal cell development and proliferation, adequate iodine levels may prevent fibroids from occurring.
Women with fibroids should be more vigilant about breast cancer, having regular breast exams and ultrasound for early detection of breast cancer.
7. Advances in Surgical Treatment
Traditional surgical treatments for fibroids are:
Removing the whole womb including the fibroids (a hysterectomy). This is an option for women who do not want to have any (more) children.
Removing the fibroids only (called myomectomy). This type of operation is suitable for women who want to keep their uterus – mainly to preserve the chance for future pregnancy.
More recent surgical treatments for fibroids include:
Removing the fibroid through keyhole surgery (laparoscopic myomectomy).
Blocking the blood vessels feeding the fibroids (uterine artery embolization) which does not remove fibroids but can cause them to shrink and reduce heavy periods.
Some fibroids that are growing inside the the womb can be removed through a hysteroscope passed inside the womb through the cervix.
There are many factors to consider when deciding the best way of removing fibroids. These include the number of fibroids, their size and exactly where they are in the womb. There can also be other issues to consider like whether you have had any operations on the womb in the past. For example, some of the fibroids that grow inside the womb can be removed by using hysteroscope operations. The fibroids that are more embedded in the womb itself cannot be removed this way.
In the last few years some hospitals have been offering SONATA: Sonography-Guided Transcervical Fibroid Ablation. It is an incisionless, uterus-preserving, transcervical approach, with real-time visualisation using intrauterine ultrasound guidance, and combines ultrasound imaging with radiofrequency energy.
Recently scientists have been developing a new therapeutic treatment using a drug capable of breaking fibroids down inside the body. Since fibroids are collagen-based, the key ingredient in this intervention is collagenase, an enzyme that digests collagen, and it is combined with LiquoGel™, which is liquid at room temperature, and becomes a gel at body temperature. Because of that, once it gets injected into a fibroid, it becomes a gel. Over time, collagenase will degrade the fibroid and LiquoGel™ will degrade, allowing the body to get rid of it. Much work remains before the treatment can reach patients.
8. Tests to Consider for Evaluation Fibroids
Transvaginal and abdominal ultrasonography
To determine the size and location of fibroids and rule out ovarian tumors
Progesterone/estradiol ratio (100–300:1) Luteal phase progesterone measurement
Low luteal phase progesterone level support oestrogen dominance and fibroid growth
Vitamin D test
Low levels increase fibroid growth by several mechanisms
Vitamin A test
Low levels shown to increase heavy bleeding
Iron or total iron-binding capacity measurement, ferritin tests
Low iron stores reduce uterine contractions and increase menstrual blood loss
Zinc and copper tests
An imbalanced copper:zinc ratio can lead to fibroids
Thyroid function testing
Hypothyroidism associated with menstrual dysfunction
MTFHR testing
35% weakness in methylation, increased oestrogen dominance
DUTCH testing for Phase 1 and Phase 2 oestrogen detoxification evaluation
Unhealthy oestrogen metabolism contributes to oestrogen dominance
Comprehensive digestive stool analysis
Intestinal dysbiosis is a cause of oestrogen dominance through several mechanisms
Vaginal microbiome testing
An unbalanced vaginal microbiome has been associated with fibroids
Testing for celiac disease (antigliadin antibodies)
Gluten grain sensitivity common in fibroid sufferers and can lead to further oestrogen dominance
9. My approach to treating fibroids
My personal experience with fibroids, and supporting women with fibroids, clearly shows that nutrition, supplements and lifestyle changes can make a significant impact on fibroid size, heavy bleeding and pain to the point of not creating any symptoms. I initially ask clients to commit to a 3-month trial period, during which they will do as much of their protocol as possible. At the end of these first 3 months, we assess symptoms, such as heavy bleeding and pain, and any growth or shrinkage of the fibroids. The protocol is considered successful if the client perceives a reduction in symptoms and no further fibroid growth has occurred. We then continue the program for 3-month periods while continuing to monitor symptoms and uterine size. If at any time symptoms recur or worsen or the fibroids begin to grow, other more aggressive measures must be considered.
Nutrition
Women with fibroids begin a hormone-balancing diet involving foods with low inflammation effects, low acidity, and a low glycemic load.
Reduce foods that increase oestrogen dominance:
Foods that are acidic and inflammatory, like red meat, poultry, and dairy, contain arachidonic acid. This acid can increase inflammation and help fibroids grow. Avoiding commercial meat products also reduces exposure to added hormones. Small amounts of range-fed meats can be added back once inflammation goes down.
Sweets and high glycemic foods can cause stress and raise insulin. This can increase oestrogen dominance and help fibroids grow. Eating breakfast with protein, fat and quality carbs prevents drops in blood sugar. This avoids spikes in cortisol and adrenaline, which break down muscle and raise insulin resistance.
Gluten grains like wheat, rye and barley contain a strong gluten that is genetically engineered. This gluten can raise oestrogen by blocking the detoxifying cytochrome P450 3A4 enzyme system. It can also affect thyroid hormones. Anyone with high oestrogen should be tested for gluten sensitivity.
Alcohol, dairy, coffee, artificial ingredients, colours, flavours and preservatives should be avoided. Also avoid margarines and foods with trans fats or hydrogenated oils.
Include foods that reduce oestrogen dominance:
Cruciferous vegetables such as broccoli, Brussels sprouts, cabbage, and cauliflower support healthy oestrogen metabolism.
3 cups of green tea daily are helpful (to reduce COMT activity).
Gut and Vaginal Microbiome Restoration, and Detoxification
Healing intestinal and vaginal microbiome imbalance and supporting liver detoxification restores hormone balance and remove sources of inflammation.
Supplements
These nutrients to support hormone metabolism and reduce inflammation:
Vitamin B complex, methylated
Vitamin D
Vitamin A
Indole-3-carbinol or diindolylmethane (DIM) to reduce estrogen dominance
Aromatase inhibitors such as Myomin can reduce oestrogen dominance
Calcium D glucarate can reduce increased recirculation of oestrogens from the gut back into the body
Iodine
Calcium: significant negative associations have been found between low serum calcium levels and uterine fibroids, uterine size and the number of fibroid nodules, possibly reflecting associated low vitamin D levels
Selenium has been shown to reduce fibroid size, possibly because it is an integral part of the antioxidant enzymes glutathioneperoxidase, catalase, and superoxide dismutase (SOD) which neutralise oxidative toxic intermediates, and of which there is a deficiency in fibroids.
Connecting women, science and spirit, the Gynelogic Sunday Supplement delivers a bi-monthly dose of news, views and reviews, as seen through my lady lens.